
Proviron New Insights

P roviron New Insights
roviron New Insights
A new blogpost about an old steroid, why? I was researching compounds that influence the libido, directly or with conjunction with other compounds. Than one of my clients told me he also used Proviron with Sustanon as HRT, especially because positively influenced his sex-life and worked well with the Sustanon. Discussing it with another friend that runs a gym and prepares men and woman for contests, he also told me he liked mesteronole (Proviron) very much and used it for diverse reasons but especially in contest preparation.
T hat made me think of my too early deceased friend Harry, people that still follow what I write sinceBody of Science, hopefully remember him. I published a lot about his drug use. Harry lived his life with an obsession for his body, looks and sexual performance. He didn’t discriminate in that regard, and made love to men and women. He was also an actor in porn movies. Thus he was an expert in what worked or didn’t work for him, mostly or actually always poly-pharmaceutic. And he also used 150 mg mesterolone per day on times he needed it. He told me it increased his ejaculate volume, and also it increased his pleasure in orgasm and his overall libido. So yes, let’s see what changed in our thoughts about mesterolone and relevant research.
hat made me think of my too early deceased friend Harry, people that still follow what I write sinceBody of Science, hopefully remember him. I published a lot about his drug use. Harry lived his life with an obsession for his body, looks and sexual performance. He didn’t discriminate in that regard, and made love to men and women. He was also an actor in porn movies. Thus he was an expert in what worked or didn’t work for him, mostly or actually always poly-pharmaceutic. And he also used 150 mg mesterolone per day on times he needed it. He told me it increased his ejaculate volume, and also it increased his pleasure in orgasm and his overall libido. So yes, let’s see what changed in our thoughts about mesterolone and relevant research.
Mesterolone is one of the oldest anabolic steroids dating back to the 1930 years, along with methyl testosterone and testosterone propionate, even these steroids are still in use. The mesterolone applications are still not sufficiently well known, as is evident by several recent studies. In the beginning, these steroids were used to enhance the wellbeing of older men and also to improve mood and overall quality of life.
A group of Brazilian researchers, sometimes supplemented with American researchers, led by Karina Fontana, conduct a series of studies on effects of mesterolone in different groups of mice. These studies have been designed to procure more insights about the consequences of what they think, supra physiological doses of anabolic steroids in the form of mesterolone. Why mesterolone and not testosterone, the prototype of anabolic androgenic steroids? This has a number of reasons, * 1 oral bioavailability and * 2 no hepatoxicity * 3 no injection induced wound-formation or liver damage that would skew the results.
I know many readers hate scientific studies, especially if they are done on mice or rats. This group of researchers however, are using specially bred mice. The results are remarkable and often contradict the prevailing bro-science rhetoric that sounds so clear on the various discussion forums. Just take the time to read the abstracts and conclusions.
Adverse effect of the anabolic–androgenic steroid mesterolone on cardiac remodelling and lipoprotein profile is attenuated by aerobicz exercise training Karina Fontana, Helena Coutinho Franco Oliveira, Marta Beatriz Leonardo, Carlos Alberto Mandarim-de-Lacerda, and Maria Alice da Cruz-Höfling 2008:
“Abuse of anabolic–androgenic steroids (AAS) for improving physical performance is associated with serious, sometimes fatal, adverse effects. The aim of the present work was to investigate the effects of AAS on the cardiac structure and the plasma lipoprotein profile isolated and in combination with exercise.
S edentary and exercised mice (treadmill running, five times per week for 6 weeks) were treated with mesterolone (2 μg/g body weight) or vehicle (control-C).
edentary and exercised mice (treadmill running, five times per week for 6 weeks) were treated with mesterolone (2 μg/g body weight) or vehicle (control-C).
Exercise training induced beneficial effects, such as physiological cardiomyocyte hypertrophy, increase in myocardial circulation and decrease in cardiac interstitium. However, mesterolone impaired such physiological gains and in addition increased troponin T plasma levels both in sedentary and exercised mice. Thus, while mesterolone induced pro-atherogenic lipoprotein profile and pathogenic cardiac hypertrophy, exercise counteracted these effects and modified favourably both the lipoprotein profile and the cardiac remodelling induced by mesterolone.”
Hepatocyte nuclear phenotype: the cross-talk between anabolic androgenic steroids and exercise in transgenic mice. Fontana K, Aldrovani M, de Paoli F, Oliveira HC, de Campos Vidal B, da Cruz-Höfling MA 2008
“The growing and indiscriminate use of high doses of anabolic androgenic steroid (AAS) among youth and athletes has raised serious concerns about its hepatotoxic effects. Herein, the influence of AAS in the nuclear phenotype of hepatocytes was investigated in sedentary and trained mice, heterozygous for the human. Five groups were assayed comprising treadmill exercised (Ex) and sedentary (Sed) mice, administered mesterolone (AAS) or gum arabic (GA) and a sedentary blank control. In this study, the image analysis permitted the monitoring of the nuclear response to mesterolone and physical exercise action in liver cells, the molecular mechanism of which is in prospect.
In conclusion, the present study is pioneering in demonstrating that the chronic use of mesterolone affects dynamically the status of chromatin condensation and texture, geometric parameters and Feulgen-DNA values in hepatocyte nuclei of sedentary and trained mice.
Mesterolone induced in sedentary mice the highest Feulgen-DNA content, which we credited both to the higher number of polyploidy cells and unpackaging of the chromatin associated to the highest increase of the nuclear size. The assessment of nuclear phenotype by image analysis can give clues to the mechanisms underlying the effects of AAS and its interplay with exercise effects in transcriptional activation or repression of eukaryotic genes. This study using a human-like lipemic mouse strain is part of a comprehensive study aimed to further understand the effects of AAS abuse.
We believe that this study will allow us to continue investigations to understand the mechanisms by which gene alterations and/or epigenetic factors provoked by the use of AAS may be linked with hepatocellular dysfunction.
In a recent study, we showed that the androgenic anabolic steroid mesterolone caused adverse cardiac remodeling and serious atherogenic lipoprotein profile in sedentary transgenic mice which express the human cholesteryl ester transfer protein (CETP) and are a
knockout for the low-density lipoprotein receptor (LDLr) (Fontana et al., 2008). In contrast, in mesterolone administered-treadmill exercised mice, the unfavorable cardiac remodeling and lipoprotein profile was markedly blunted.”
Effect of high intensity aerobic exercise and mesterolone on remodeling of Achilles tendon of C57BL/6 transgenic mice Fontana et all 2010:
“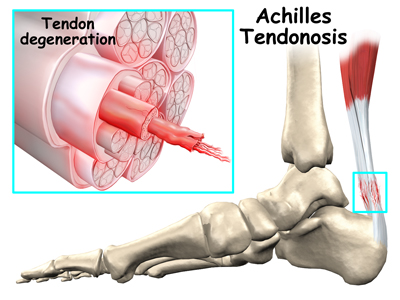 The effect of mesterolone and intensive treadmill training (6 weeks, 5 days/week, means: 15.82 m/min and 45.8 min/day) in Achilles tendon remodeling was evaluated. Sedentary mice treated with mesterolone or vehicle (placebo) and corresponding exercised (with mesterolone and without) were examined.”
The effect of mesterolone and intensive treadmill training (6 weeks, 5 days/week, means: 15.82 m/min and 45.8 min/day) in Achilles tendon remodeling was evaluated. Sedentary mice treated with mesterolone or vehicle (placebo) and corresponding exercised (with mesterolone and without) were examined.”
Conclusion:“Thus, mechanical stimuli <and mesterolone alter the morphology of tenocytes and the composition of the tendon, probably through fibrillogenesis and/or increased intermolecular cross-links. The ergogenic effect is evidenced by the activation of collagenous and non-collagenous protein synthesis and the increase in the diameter and area of collagen fibrils. This study might be relevant to clinical sports medicine<.”
Morphological changes in murine skeletal muscle in response to exercise and mesteroloneFontana K, White KE, Campos GE, da Cruz-Höfling MA, Harris JB. 2010:
“Light and electron microscopy and quantitative morphometry were used to determine the effects of exercise and mesterolone on the soleus muscles of mice. Both exercise and mesterolone caused a significant hypertrophy of extrafusal muscle fibres. The hypertrophy of Type I fibres was greater than that of Type II fibres. There was no hyperplasia. Mitochondria were more numerous and larger than in the muscles of sedentary animals. Capillarity increased and small centrally nucleated muscle fibres appeared, usually in small clusters and most often in the muscles of animals exposed to mesterolone. A small proportion of satellite cells exhibited signs of activation but there were more in the muscles of mesterolone-treated animals than after exercise. Muscles from animals that had been both exercised and treated with mesterolone exhibited the largest changes: muscle mass and muscle fibre hypertrophy was greater than in all other groups of animals, capillarity was higher and >30% of all recognized satellite cells exhibited signs of activation.”
Groups of small centrally nucleated muscle fibres were commonly seen in these muscles. They appeared to be the result of splits in the form of sprouts from existing muscle fibres. With both exercise and mesterolone, alone or in combination, there was an increase in the proportion of Type I muscle fibres and a decrease in the proportion of Type II.”
Regulation of neuronal and endothelial nitric oxide synthase by anabolic-androgenic steroid in skeletal muscles K Fontana, T Rocha, MA da Cruz-Hoefling 2012
“Anabolic-androgenic steroids (AAS) and exercise share comparable effects on myogenic differentiation, force development, fiber growth and skeletal muscle plasticity. The participation of nitric oxide synthase (NOS) on these effects was only demonstrated in response to exercise. Using immunohistochemistry and western blotting we examined the effect of AAS on the expression of NOS I and III isoforms in three muscles.
Mice with a lipid profile akin to humans were used. Sedentary mice or exercised, submitted to six-weeks of aerobic treadmill running (one hour/day, 5 days/week) were administered mesterolone.
Mesterolone administered to sedentary mice significantly upregulated NOS I in TA and SOL and NOS III in all three muscles. Mesterolone administered to exercised mice upregulated NOS I in all three muscles and NOS III in TA and SOL. The exercise to mesterolone-treated mice produced a strong increase in NOS I expression.
These may be regarded as an indication of the complex NOS/NO signaling mechanism related with AAS effects vs. metabolic/physiological muscle characteristics.”
Effects of Anabolic Steroids and High-Intensity Aerobic Exercise on Skeletal Muscle of Transgenic Mice Fontana et all 2013
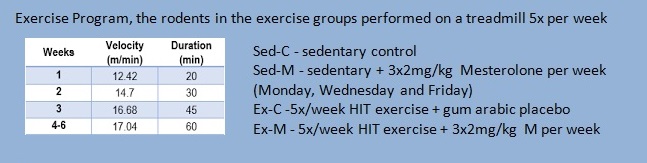
I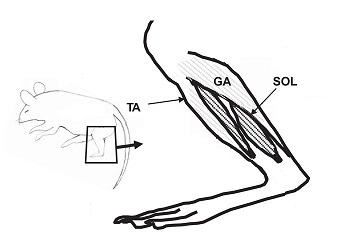 n a 6-week rodent study, Brazilian scientists Karina Fontana, Gerson E. R. Campos, Robert S. Staron and Maria Alice da Cruz-Höfling undertook a study to examine the effects of mesterolone (1-alpha-methylated-DHT or Proviron®), on the fiber type composition and cross-sectional area of skeletal muscle fibers of sedentary and high-intensity, aerobically-exercised transgenic mice. Thus, the aim was to investigate the role of mesterolone in a supposed catabolic environment. Does the interaction of anabolic hormone treatment and high-intensity aerobic exercise (HIT) produce an increase in muscle mass and redistribution of skeletal muscle fiber types? Are muscles with distinct metabolic and contractile properties (i.e. fast/glycolytic vs. slow/oxidative) differently modulated by the anabolic androgenic steroid treatment combined with a high-intensity, endurance-type training program?
n a 6-week rodent study, Brazilian scientists Karina Fontana, Gerson E. R. Campos, Robert S. Staron and Maria Alice da Cruz-Höfling undertook a study to examine the effects of mesterolone (1-alpha-methylated-DHT or Proviron®), on the fiber type composition and cross-sectional area of skeletal muscle fibers of sedentary and high-intensity, aerobically-exercised transgenic mice. Thus, the aim was to investigate the role of mesterolone in a supposed catabolic environment. Does the interaction of anabolic hormone treatment and high-intensity aerobic exercise (HIT) produce an increase in muscle mass and redistribution of skeletal muscle fiber types? Are muscles with distinct metabolic and contractile properties (i.e. fast/glycolytic vs. slow/oxidative) differently modulated by the anabolic androgenic steroid treatment combined with a high-intensity, endurance-type training program?
As such, three skeletalmuscles were studied under these experimental conditions: soleus (SOL), tibialis anterior (TA) and gastrocnemius (GA).
The animals either received gum arabic or the dihydrotestosterone derivative, mesterolone (M) (2 mg/kg body weight), during the last 3 weeks of the study (3d/wk: Monday, Wednesday, and Friday). The amount of mesterolone administered per week (6 mg/kg) is considered to be a high dose (supra-therapeutic) and is comparable to doses reportedly used in humans.
What the researchers believe to be supra-therapeutic (or unusual high dose) is in fact an unusual low dose.< The rodents receive 3x2mg/kg Mesterolone per week on Monday, Wednesday and Friday. HUMAN EQUIVALENT DOSE (HED) = 2 mg/ kg for a mouse = 2 x [3 / 37] = 0.162 mg/kg, for a 100 kg athlete that is 16 mg. Bodybuilders and athletes normally use 50-150 mg/day.
Mesterolone (1 alpha-methyl-17 beta-hydroxy-5 alpha-androstan-3-one) was chosen for three reasons: it can be administered orally avoiding injection induced wound formation and as a non-17 alpha-alkylated derivative of testosterone it presents low hepatotoxicity.
Overall, it is difficult to explain such varied findings concerning the effects of AAS treatment on fiber type distribution and size. Conflicting evidence may be due to a variety of factors: species, muscles chosen, androgen receptor density, fiber typing methodology, dosage/type of AAS, mode of administration, study duration, gender, age, and activity level.
I n the present study, we were able to detect subtle changes in fiber type distribution with the utilization of refined mATPase histochemistry by delineating the entire range of pure/hybrid fiber types. Previous AAS studies have separated fibers into either two or three broad categories, and were thus, likely unable to detect subtle changes in fiber type composition. Data from the present study suggest a differential AAS response between slow and fast muscles. Mesterolone induced differential adaptive changes in the transgenic mice hindlimb muscles amounting to significant fast-to-slow fiber type transformations in the slow soleus muscle with minimal effect on the predominantly fast muscles<
n the present study, we were able to detect subtle changes in fiber type distribution with the utilization of refined mATPase histochemistry by delineating the entire range of pure/hybrid fiber types. Previous AAS studies have separated fibers into either two or three broad categories, and were thus, likely unable to detect subtle changes in fiber type composition. Data from the present study suggest a differential AAS response between slow and fast muscles. Mesterolone induced differential adaptive changes in the transgenic mice hindlimb muscles amounting to significant fast-to-slow fiber type transformations in the slow soleus muscle with minimal effect on the predominantly fast muscles<
Mesterolone and exercise each induced comparable increases in the size of all major fiber types in all three muscles. However, AAS plus exercise caused a cumulative effect resulting in additional hypertrophy.
These data were supported by similar increases in the muscle wet weights. The findings show that in this transgenic murine model the caloric expenditure induced by a metabolically-demanding exercise program was superimposed by protein synthesis resulting in muscle mass gains, which were potentiated in trained animals treated with mesterolone. Data obtained from this transgenic model (specifically engineered to express a lipemic phenotype akin to humans) could be relevant to humans from a comparative perspective.
How does mesterolone induce muscle growth?
Influence of mesterolone on satellite cell distribution and fiber morphology within maturing chicken pectoralis muscle Allouh et all 2012:<
“Mesterolone is a synthetic oral anabolic androgenic steroid used to treat hypogonadism. There are frequent reports of mesterolone abuse in human and equine sports to increase muscle mass and strength. However, limited information is available about how this drug exerts its effects on skeletal muscle. Satellite cells (SCs) are mononuclear myogenic stem cells that contribute to postnatal muscle growth and repair. As SC activation and subsequent differentiation to new myonuclei is a major event during muscle hypertrophy.
This study indicates that mesterolone can induce avian skeletal muscle hypertrophy and that this is correlated with increased number of Satellite cells. We suggest that Satellite cells are key cellular intermediaries for mesterolone-induced muscle hypertrophy.”
Mesterolone treatment of aging male syndrome improves lower urinary tract symptoms Dugeroglu et all 2014
Their objective was to investigate the effects of mesterolone on prostate in patients treated for aging male syndrome. Their conclusion: “Mesterolone proved to be a safe alternative in the treatment of Aging Male Syndrome. It also improved lower urinary tract symptoms and prostate-related quality of life.”
Newer research indeed suggests mesterolone to improve mood.
 A comparison of the antidepressant effects of mesterolone and amitriptyline in depressed men, showed the drugs were equally effective in reducing depressive symptoms. But mesterolone produced significantly fewer adverse side effects than amitriptyline.”
A comparison of the antidepressant effects of mesterolone and amitriptyline in depressed men, showed the drugs were equally effective in reducing depressive symptoms. But mesterolone produced significantly fewer adverse side effects than amitriptyline.”
From the same study: "Nowadays it is well known that one of the main physiological functions of testosterone is to tune up erection with sexual desire, finalizing erection to emotional processing. Testosterone replacement therapy (TRT) has been described to significantly improve cognitive function in the general population, and also in the depressed men. More recently, also the negative symptoms in male schizophrenic patients have been correlated with serum testosterone level and short-term testosterone treatment has been suggested as a therapeutic option in male schizophrenics. "
Most guys hate to excerpts from scientific studies, but I’ll think you need to see this one:
The effects of mesterolone on sperm count in idiopathic oligospermia. Bhathena et all: “Forty subfertile men with idiopathic oligospermia were randomly treated with mesterolone or with placebo for more than 4 months. Seminal analysis was performed thrice before treatment, and twice after 16 weeks of treatment. There was a significant increase of semen volume, mean sperm concentration, and mean total sperm count per ejaculate (P less than .01) with mesterolone therapy.”
Mesterolone for Women
Long-term treatment of renal anaemia with mesterolone. Kraft D 1980:
 “Mesterolone, 150 mg daily by mouth, was given to 26 patients (10 men, 16 women) with renal anaemia on chronic haemodialysis (3 times for 5 hours). At the beginning of treatment the patients had been dialysed for at least 6 months under stable conditions: iron deficiency had been excluded or treated. Progressive improvement in the anaemia was observed during the treatment period. After 39 months the haemoglobin concentration had risen from 74 +/- 4 g/l to 95 +/- 5 g/l, haematocrit from 0.22 +/- 0.01 to 0.28 +/- 0.02, and the red-cell count from 2.44 +/- 0.12 X 10(12)/l to 3.09 +/- 0.2 X 10(12)/l. Side effects were rare; some patients developed increased appetite with a rise in body weight, while some women developed acne or hirsutism. There was no effect of mesterolone on liver function. The results indicate that mesterolone can favourably influence renal anaemia and that the side effects of this testosterone derivative are not such as to prohibit its use in women.”
“Mesterolone, 150 mg daily by mouth, was given to 26 patients (10 men, 16 women) with renal anaemia on chronic haemodialysis (3 times for 5 hours). At the beginning of treatment the patients had been dialysed for at least 6 months under stable conditions: iron deficiency had been excluded or treated. Progressive improvement in the anaemia was observed during the treatment period. After 39 months the haemoglobin concentration had risen from 74 +/- 4 g/l to 95 +/- 5 g/l, haematocrit from 0.22 +/- 0.01 to 0.28 +/- 0.02, and the red-cell count from 2.44 +/- 0.12 X 10(12)/l to 3.09 +/- 0.2 X 10(12)/l. Side effects were rare; some patients developed increased appetite with a rise in body weight, while some women developed acne or hirsutism. There was no effect of mesterolone on liver function. The results indicate that mesterolone can favourably influence renal anaemia and that the side effects of this testosterone derivative are not such as to prohibit its use in women.”
Which made a girl rave on a discussion forum: “Hirsutism is NOT wanted, but this was a dose of 150mg, whereas 10-25mg will be enough to get the libido racing ![]()
![]()
![]()
![]() ”
”
A nice set of studies on axis suppression I found on the net:
S uppression From Standalone Proviron
uppression From Standalone Proviron
This thread is regarding Proviron used standalone for non-cycle, non-PCT purposes such as strength gain or aggression in the weight room, libido, muscle hardening, etc. I've often wondered if suppression would become a significant issue when it's used for sometimes prolonged periods in someone with a normal hormonal environment, and if PCT is necessary when using it like this. I've complied a group of studies to find out.
#1 : The effect of mesterolone on sperm count, on serum follicle stimulating hormone, luteinizing hormone, plasma testosterone and outcome in idiopathic oligospermic men.
Two hundred fifty subfertile men with idiopathic oligospermia (count less than 20 million/ml) were treated with mesterolone (100-150 mg/day) for 12 months. Seminal analysis were assayed 3 times and serum follicle stimulating hormone (FSH) luteinizing hormone (LH) and plasma testosterone were assayed once before treatment and repeated at 3, 6, 9 and 12 months after the initiation of treatment. One hundred ten patients (44%) had normal serum FSH, LH and plasma testosterone, 85 patients (34%) had low serum FSH, LH and low plasma testosterone. One hundred seventy-five patients (70%) had moderate oligospermia (count 5 to less than 20 million/ml) and 75 patients (30%) had severe oligospermia (count less than 5 million/ml). Seventy-five moderately oligospermic patients showed significant improvement in the sperm density, total sperm count and motility following mesterolone therapy whereas only 12% showed improvement in the severe oligospermic group. Mesterolone had no depressing effect on low or normal serum FSH and LH levels but had depressing effect on 25% if the levels were elevated. There was no significant adverse effect on testosterone levels or on liver function. One hundred fifteen (46%) pregnancies resulted following the treatment, 9 of 115 (7.8%) aborted and 2 (1.7%) had ectopic pregnancy. Mesterolone was found to be more useful in patients with a sperm count ranging between 5 and 20 million/ml. Those with severe oligospermia (count less than 5 million) do not seem to benefit from this therapy.
NOTES: Used a large group, most of whom were hormonally normal. LH lowered a bit if it was elevated, but not really relevant because testosterone levels showed no significant change in all subjects anyways.
_________________________________________________________
#2 :Mesterolone treatment of patients with pathospermia.
The response to Mesterolone, in doses of 25 mg/day, was examined in 42 pathospermic patients. Treatment lasted for 100 days. The pronounced response to the Mesterolone treatment was observed in hypozoo- and oligozoospermia with low initial fructose content in the ejaculate. Fructose content attained its normal range after the treatment. During the therapeutic period 11 wives became pregnant. The authors conclude that Mesterolone does not influence plasma FSH, LH and testosterone levels, it has only peripheral effects.
NOTES: Low dose over a decent 3 month time frame. No measurable influence on HPTA.
_________________________________________________________
#3 : Plasma cholesterol, triglycerides, FSH and testosterone levels of normolipemic male patients with decreased fertility treated with mesterolone.
There were no changes in plasma cholesterol, triglycerides, FSH and testosterone levels of 24 healthy men treated with mesterolone for infertility during period of 6 months. The patients were normolipemic and the daily doses were 75 mg. No side-effects were noticed. Mesterolone seems to have too selective or too low androgenic effect with the doses used in orde to have an influence on the lipid metabolism of men.
NOTES: Decent sized group, again healthy, apart from being infertile. Low-medium dose for a pretty long time period. Again no significant suppression.
__________________________________________________________
# 4: The effects of mesterolone on the male accessory sex organs, on spermiogram, plasma testosterone and FSH.
42 subfertile male ambulatory patients were treated with Proviron. Moderate oligoastheno-teratozoospermia was the most common injury in sperm analysis. The treatment did not change the amount of plasma FSH, testosterone or prostate phosphatase. Acid phosphatase and citric acid of semen showed an increased activity with mesterolone treatment. The amount of fructose decreased, it is probably due to the increased number of spermatozoa, which need more fructose for their metabolism respectively. The sperm of 93% of the patients improved or stayed unchanged. 30% of the patients developed normozoospermia. 6 pregnancies were achieved.
NOTES: Here, as well as being infertile, the patients are also bedridden. The reasons for this are not given. Nor is the daily dose amount of mesterolone. By itself, this study is hardly anything at all, but taken together with the above studies which also failed to detect endocrine changes, it can be suggestive and so should be considered. __________________________________________________________
#5 : Effect of non aromatizable androgens on LHRH and TRH responses in primary testicular failure. We have assessed the gonadotropin, TSH and PRL responses to the non aromatizable androgens, mesterolone and fluoxymestrone, in 27 patients with primary testicular failure. All patients were given a bolus of LHRH (100 micrograms) and TRH (200 micrograms) at zero time. Nine subjects received a further bolus of TRH at 30 mins. The latter were then given mesterolone 150 mg daily for 6 weeks. The remaining subjects received fluoxymesterone 5 mg daily for 4 weeks and 10 mg daily for 2 weeks. On the last day of the androgen administration, the subjects were re-challenged with LHRH and TRH according to the identical protocol. When compared to controls, the patients had normal circulating levels of testosterone, estradiol, PRL and thyroid hormones. However, basal LH, FSH and TSH levels, as well as gonadotropin responses to LHRH and TSH and PRL responses to TRH, were increased. Mesterolone administration produced no changes in steroids, thyroid hormones, gonadotropins nor PRL. There was, however, a reduction in the integrated and incremental TSH secretion after TRH. Fluoxymesterone administration was accompanied by a reduction in thyroid binding globulin (with associated decreases in T3 and increases in T3 resin uptake). The free T4 index was unaltered, which implies that thyroid function was unchanged. In addition, during fluoxymesterone administration, there was a reduction in testosterone, gonadotropins and LH response to LHRH. Basal TSH did not vary, but there was a reduction in the peak and integrated TSH response to TRH. PRL levels were unaltered during fluoxymesterone treatment.
We have assessed the gonadotropin, TSH and PRL responses to the non aromatizable androgens, mesterolone and fluoxymestrone, in 27 patients with primary testicular failure. All patients were given a bolus of LHRH (100 micrograms) and TRH (200 micrograms) at zero time. Nine subjects received a further bolus of TRH at 30 mins. The latter were then given mesterolone 150 mg daily for 6 weeks. The remaining subjects received fluoxymesterone 5 mg daily for 4 weeks and 10 mg daily for 2 weeks. On the last day of the androgen administration, the subjects were re-challenged with LHRH and TRH according to the identical protocol. When compared to controls, the patients had normal circulating levels of testosterone, estradiol, PRL and thyroid hormones. However, basal LH, FSH and TSH levels, as well as gonadotropin responses to LHRH and TSH and PRL responses to TRH, were increased. Mesterolone administration produced no changes in steroids, thyroid hormones, gonadotropins nor PRL. There was, however, a reduction in the integrated and incremental TSH secretion after TRH. Fluoxymesterone administration was accompanied by a reduction in thyroid binding globulin (with associated decreases in T3 and increases in T3 resin uptake). The free T4 index was unaltered, which implies that thyroid function was unchanged. In addition, during fluoxymesterone administration, there was a reduction in testosterone, gonadotropins and LH response to LHRH. Basal TSH did not vary, but there was a reduction in the peak and integrated TSH response to TRH. PRL levels were unaltered during fluoxymesterone treatment.
This is what you normally find on the net about Proviron (mesterolone):
M esterolone has four distinct uses in the world of bodybuilding. The first being the result of its structure. It is 5-alpha reduced and not capable of forming estrogen, yet it nonetheless has a much higher affinity for the aromatase enzyme (which converts testosterone to estrogen) than testosterone does. That means in administering it with testosterone or another aromatizable compound, it prevents estrogen build-up because it binds to the aromatase enzyme very strongly, thereby preventing these steroids from interacting with it and forming estrogen.
esterolone has four distinct uses in the world of bodybuilding. The first being the result of its structure. It is 5-alpha reduced and not capable of forming estrogen, yet it nonetheless has a much higher affinity for the aromatase enzyme (which converts testosterone to estrogen) than testosterone does. That means in administering it with testosterone or another aromatizable compound, it prevents estrogen build-up because it binds to the aromatase enzyme very strongly, thereby preventing these steroids from interacting with it and forming estrogen.  So Mesterolone use has the extreme benefit of reducing estrogenic side-effects and water retention noted with other steroids, and as such still help to provide mostly lean gains. It’s also been suggested that it may actually downgrade the actual estrogen receptor making it doubly effective at reducing circulating estrogen levels.
So Mesterolone use has the extreme benefit of reducing estrogenic side-effects and water retention noted with other steroids, and as such still help to provide mostly lean gains. It’s also been suggested that it may actually downgrade the actual estrogen receptor making it doubly effective at reducing circulating estrogen levels.
The second use is in enhancing the potency of testosterone. Testosterone in the body at normal physiological levels is mostly inactive. As much as 97 or 98 percent of testosterone in that amount is bound to sex hormone binding globulin (SHBG) and albumin, two proteins. In such a form testosterone is mostly inactive. But as with the aromatase enzyme, DHT has a higher affinity for these proteins than testosterone does, so when administered simultaneously the mesterolone will attach to the SHBG and albumin, leaving larger amounts of free testosterone to mediate anabolic activities such as proteinsynthesis. Another way in which it helps to increase gains. It’s also another part of the equation that makes it ineffective on its own, as binding to these proteins too, would render it a non-issue at the androgen receptor.
Thirdly, mesterolone is added in pre-contest phases to increase a distinct hardness and muscle density. Probably due to its reduction in circulating estrogen, perhaps due to the downregulating of the estrogen receptor in muscle tissue, it decreases the total water build-up of the body giving its user a much leaner look, and a visual effect of possessing "harder" muscles with more cuts and striations. Proviron is often used as a last-minute secret by a lot of bodybuilders and both actors and models have used it time and again to deliver top shape day in day out, when needed. Like the other methylated DHT compound, drostanolone, mesterolone is particularly potent in achieving this feat.
Lastly Proviron is used during a cycle of certain hormones such as nandrolone, with a distinct lack of androgenic nature, or perhaps 5-alpha reduced hormones that don't have the same affinities as DHT does. Such compounds, thinking of trenbolone, nandrolone and such in particular, have been known to decrease libido. Limiting the athlete to perform sexually being the logical result. DHT plays a key role in this process and is therefore administered in conjunction with such steroids to ease or relieve this annoying side-effect. Proviron is also commonly prescribed by doctors to people with low levels of testosterone, or patients with chronic impotence. It’s not perceived as a powerful anabolic, but it gets the job done equally well if not better than other anabolic steroids making it a favorite in medical practices due to its lower chance of abuse.
