
Oxandrolone

 Anavar was the old U.S. brand name for the oral steroid oxandrolone, is a drug created by Searle Laboratories, now Pfizer Inc, and introduced into the US in 1964. Oxandrolone is a synthetic anabolic steroid derived from dihydrotestosterone (DHT) by substituting the second carbon atom for oxygen. The drug was prescribed to promote muscle regrowth in disorders which cause involuntary weight loss. It had also been shown to be partially successful in treating cases of osteoporosis. Recently, it was approved as a drug in treating alcoholic hepatitis, Turner syndrome, and weight loss caused by HIV. It is also indicated as an offset to protein catabolism caused by long-term administration of corticosteroids. In addition, the drug has shown positive results in treating anemia and hereditary angioedema.
Anavar was the old U.S. brand name for the oral steroid oxandrolone, is a drug created by Searle Laboratories, now Pfizer Inc, and introduced into the US in 1964. Oxandrolone is a synthetic anabolic steroid derived from dihydrotestosterone (DHT) by substituting the second carbon atom for oxygen. The drug was prescribed to promote muscle regrowth in disorders which cause involuntary weight loss. It had also been shown to be partially successful in treating cases of osteoporosis. Recently, it was approved as a drug in treating alcoholic hepatitis, Turner syndrome, and weight loss caused by HIV. It is also indicated as an offset to protein catabolism caused by long-term administration of corticosteroids. In addition, the drug has shown positive results in treating anemia and hereditary angioedema.
But the atmosphere surrounding steroids began to change rapidly in the 1980's due to steroids in baseball scandal, and prescriptions for oxandrolone began to drop. Lagging sales probably led Searle to discontinue manufacture in 1989, and it had vanished from U.S. pharmacies. Oxandrolone tablets are again available inside the U.S. by BTG, bearing the new brand name Oxandrin. BTG purchased rights to the drug from Searle and it is now manufactured for the new purpose of treating HIV/AIDS related wasting syndrome.

On the black market, oxandrolone has always been a hot item. Although it is again being manufactured in the U.S., don't count on seeing it much. The exorbitant price BTG is asking for Oxandrin precludes it from entering the black market in any volume. At the pharmacy, these tablets can cost over $4 each, a tremendous jump from the price Searle was selling It for a decade earlier.
Anabolic steroids have truly found their niche nowadays in the muscle-building and anti-aging world. One of such substance is Oxandrolone.
Short-Term Oxandrolone Administration Stimulates Net Muscle Protein Synthesis in Young Men” SHEFFIELD-MOORE et all: Note these outcomes are not from very old and or severe sick people, but healthy young guys in their twenties. ”This suggests that Oxandrolone may exert a greater anabolic influence on skeletal muscle than Testosterone Enanthate, thereby overcoming the decrease in the Testosterone concentration. Further evidence indicates that the method of administration and metabolism of the anabolic agent may account for the magnitude of difference in protein synthesis with Oxandrolone (OX) compared to Testosterone Enanthate. For example, intra muscular (im) Testosterone Enanthate (TE) injections are administered in a lipid base such that they can be stored in adipose tissue and released slowly, giving a sustained duration of action. After im injection of 200 mg TE, serum T levels rise and can reach the supraphysiological range within 24 h of administration. Over a period of several weeks, these levels gradually decline to hypogonadal levels. In the present study, serum OX levels on day 5 were 2.19 ng/dL 10 h after oral administration. However, by 18 h, serum OX levels fell to 0.48 ng/dL, representing a 78% reduction in serum OX in only 8 h. Because of this rapid decline in OX blood levels, it may be warranted to administer OX twice a day to maintain higher sustained blood levels of total androgen, possibly further enhancing its anabolic effect on skeletal muscle.”
“More recent evidence lends support to the complementary roles of androgens, ARs, and IGF-I. Mauras et al. showed marked decreases in mRNA concentrations of IGF-I and suggested that within skeletal muscle tissue, androgens are necessary for local IGF-I production, independent of GH production and systemic IGF-I concentrations.”
Women. Oxandrolone was designed as an extremely mild anabolic, one that could even be safely used as a growth stimulant in children. One immediately thinks of the standard worry, "steroids will stunt growth". But it is actually the excess estrogen produced by most steroids that is the culprit, just as it is the reason why women stop growing sooner and have a shorter average stature than men. Oxandrolone will not aromatize, and therefore the anabolic effect of the compound can actually promote linear growth. Women usually tolerate this drug well at low doses, and at one time it was prescribed for the treatment of osteoporosis.
Women who fear the masculinizing effects of many steroids would be quite comfortable using this drug, as this is very rarely seen with low doses. Here a daily dosage of 5mg should illicit considerable growth without the noticeable androgenic side effects of other drugs. Eager females may wish to addition mild anabolics like Winstrol®, Primobolan® or Durabolin®. When combined with such anabolics, the user should notice faster, more pronounced muscle-building effects, but may also increase the likelihood of androgenic buildup.
Inhibition. Studies using low dosages of this compound note minimal interferences with natural testosterone production. Likewise when it is used alone in small amounts there is typically no need for ancillary drugs like Clomid®/Nolvadex® or HCG. This has a lot to do with the fact that it does not convert to estrogen, which we know has an extremely profound effect on endogenous hormone production. Without estrogen to trigger negative feedback, we seem to note a higher threshold before inhibition is noted. But at higher dosages of course, a suppression of natural testosterone levels will still occur with this drug as with any anabolic/androgenic steroid.
Are all 17alpha alkylated steroids equally toxic, or are some worse than others? Liver damage is probably the most sensationalized of all possible side effects from oral steroid use. The media often focuses on this particular problem as if it occurs with every steroid, and in every person who takes them. Nothing could be further than the truth. Most anabolic steroids which are ingested orally pass through the liver, which functions as the body´s filtration system. When something goes through the liver, it is broken down by various enzymes, and passed along into the bloodstream. Most research on orally administered anabolic steroids focus on the fact that liver enzymes are elevated following ingestion. But does this necessarily mean that the liver is being damaged, does it? Of course not. All Oral Steroids put stress on the liver. So does alcohol, prescription drugs, anti-conception pills taken for an extended period of time, asprin and physical conditions like overweight/obesity.
 Oxandrolone is a c17-alpha alkylated compound. This alteration protects the drug from deactivation by the liver, allowing a very high percentage of the drug entry into the bloodstream following oral adminstration. C17-alpha alkylated anabolic/androgenic steroids can be hepatotoxic. Prolonged or high exposure may result in liver damage. In rare instances life threatening dysfunction may develop. It is advisable to visit a physician periodically during each cycle to monitor liver function and overall health. Intake of c17-alpha alkylated steroids is commonly limited to 6 – 8 weeks, in an effort to avoid escalating liver strain.
Oxandrolone is a c17-alpha alkylated compound. This alteration protects the drug from deactivation by the liver, allowing a very high percentage of the drug entry into the bloodstream following oral adminstration. C17-alpha alkylated anabolic/androgenic steroids can be hepatotoxic. Prolonged or high exposure may result in liver damage. In rare instances life threatening dysfunction may develop. It is advisable to visit a physician periodically during each cycle to monitor liver function and overall health. Intake of c17-alpha alkylated steroids is commonly limited to 6 – 8 weeks, in an effort to avoid escalating liver strain.
Oxandrolone appears to offer less hepatic stress than other c-17 alpha alkylated steroids. The manufacturer identifies oxandrolone as a steroid that is not extensively metabolized by the liver like other 17-alpha alkylated orals, which may be a factor in its reduced hepatotoxicity. This is evidenced by the fact that more than a third of the compound is still intact when excreted in the urine. Another study comparing the effects of oxandrolone to other alkylated agents including methyltestosterone, norethandrolone, fluoxymesterone, and methandriol demonstrated that oxandrolone causes the lowest sulfobromophthalein (BSP; a marker of liver stress) retention of the agents tested. 20mg of oxandrolone produced 72% less BSP retention than an equal dosage of fluoxymesterone, which is a considerable difference being that they are both 17-alpha alkylated.
A more recent study looked at escalating doses (20mg, 40mg, and 80mg) of oxandrolone in 262 HIV+ men. The drug was administered for a period of 12 weeks. The group taking 20mg of oxandrolone per day showed no significant trends of hepatotoxicity in liver enzyme (AST/ALT; aminotransferase and alanine aminotransferase) values. Those men taking 40mg noticed a mean increase of approximately 30 – 50% in liver enzyme values, while the group of men taking 80mg noticed an approximate 50 – 100% increase. Approximately 10 – 11% of the patients in the 40mg group noticed World Health Organization grade III and IV toxicity according to AST and ALT values. This figure jumped to 15% in the 80mg group. While serious hepatotoxicity cannot be excluded with oxandrolone, these studies do suggest that it is measurably safer than other alkylated agents.
per day showed no significant trends of hepatotoxicity in liver enzyme (AST/ALT; aminotransferase and alanine aminotransferase) values. Those men taking 40mg noticed a mean increase of approximately 30 – 50% in liver enzyme values, while the group of men taking 80mg noticed an approximate 50 – 100% increase. Approximately 10 – 11% of the patients in the 40mg group noticed World Health Organization grade III and IV toxicity according to AST and ALT values. This figure jumped to 15% in the 80mg group. While serious hepatotoxicity cannot be excluded with oxandrolone, these studies do suggest that it is measurably safer than other alkylated agents.
All oral steroids are somewhat "liver toxic" or burden the liver in a dose-related manner, and my experience is that the actual toxicity is somewhat exaggerated.
Some supplements work synergistically with Oxandrolone. After Anavar is taken, and its active in the system, it is up regulating the androgen receptor and its ability to cause Noradrenalin to bind to adrenoreceptors in fat cells, then Guanine nucleotide proteins cause the enzyme Adenylate cyclase to convert ATP into cAMP. This is why creatine and Oxandrolone work so well together as creatine increases muscle ATP.
Using Creatine with Anavar is important since Oxandrolone causes ATP to be reduced in its method of burning fat. It also has the ability to store creatine to a much greater level so consuming creatine along with Oxandrolone will cause far greater strength increases and fat loss.
cAMP then binds to the protein kinase A, then protein kinase A release its catalytic subunit, This subunit phosphorylates (HSL ) it then becomes an active enzyme, called HSL-P, Then finally a 3 step action catalytic action takes place wich causes the breakdown of tryglycerides, they are then released into the blood system and excreted.
 The body tries to prevent fat breakdown via the negative feedback loop. One way it does this with Anavar is to try and prevent the accumulation of cAMP within cells. Caffeine can be used to prevent this by inhibiting phosphodiesterases within the cell. It also can prevent the actions of adenosine, which make it very useful when used alongside Anavar at a dose of 60mg-90 mg, pre workout.
The body tries to prevent fat breakdown via the negative feedback loop. One way it does this with Anavar is to try and prevent the accumulation of cAMP within cells. Caffeine can be used to prevent this by inhibiting phosphodiesterases within the cell. It also can prevent the actions of adenosine, which make it very useful when used alongside Anavar at a dose of 60mg-90 mg, pre workout.
Can a few hundred mils of caffeine boost the anabolic effect of oxandrolone? Imagine: you're a careful user of anabolic steroids. You occasionally take a course of oxandrolone only, and that's all you want. If this is your way of doing things, then Portuguese doping researchers may have discovered something that'll interest you. They suspect that you can get more out of oxandrolone if you take extra caffeine.
The Portuguese, who work for the doping lab Laboratório de Análises de Dopagem, were tipped by the police that some Portuguese steroids users swear by a combination of caffeine and oxandrolone. The researchers were curious to know more about the potential use of this combination, so they consulted the literature.
They came across studies which show that caffeine can boost the uptake and effect of paracetamol. So, they reasoned, might caffeine have the same effect when taken with oxandrolone?
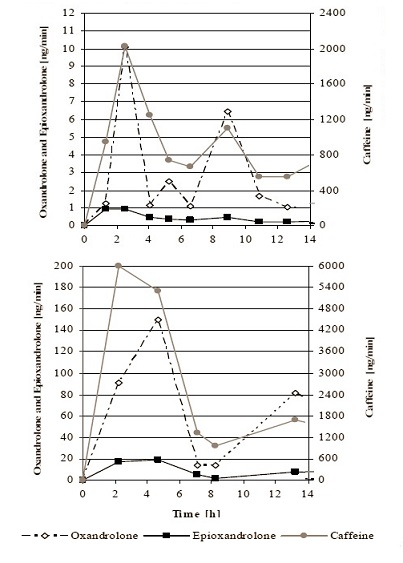
To answer this question the researchers performed an experiment in which they gave a subject, whose caffeine consumption was a normal three small espressos a day, a miniscule quantity [0.4 mg] of oxandrolone.
The researchers then monitored the amount of caffeine, oxandrolone and the inactive oxandrolone metabolite epioxandrolone in the subject's urine for the next 40 hours. The figure below shows the amounts found in the first 14 hours.
The researchers then repeated the experiment, but gave the subject 300 mg caffeine in pill form. The figure above [click on it for a complete figure] shows that the amount of oxandrolone and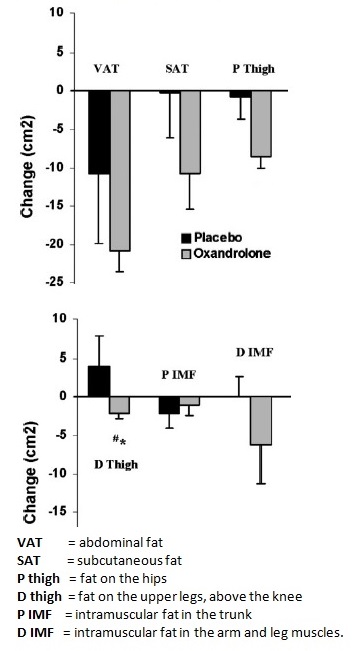 epioxandrolone rose by a factor of 20 and 15 respectively. The researchers think their experiment may show that caffeine causes a considerable improvement in the uptake of oxandrolone by the body. "Practically this means that similar concentrations/effects may be achieved using lower dosages", they write. "Other anabolic steroids should also be investigated."
epioxandrolone rose by a factor of 20 and 15 respectively. The researchers think their experiment may show that caffeine causes a considerable improvement in the uptake of oxandrolone by the body. "Practically this means that similar concentrations/effects may be achieved using lower dosages", they write. "Other anabolic steroids should also be investigated."
Oxandrolone as a slimming aid. Steroids like oxandrolone not only build muscle mass, they also break down body fat. One problem with the former effect is that much of the muscle mass that has been built up disappears once the athlete stops taking oxandrolone. According to research done in 2004 at the University of Southern California, the fat loss effect of oxandrolone does not have this drawback.
Early in the 21st century American endocrinologists, financed partly by the government and partly by oxandrolone manufacturer Savient, studied the effects of modest doses of oxandrolone on elderly men. The researchers wanted to establish how effective and safe oxandrolone really is. Although the study involved non-active men who were above 60, it did produce information that is interesting for chemical athletes.
The study showed that men gain muscle mass and lose fat mass if they take oxandrolone for 12 weeks, but also that 12 weeks further on the muscles built up have disappeared again. But the fat that was lost stays away. Most of the benefit of a course of oxandrolone is derived in the first six weeks of the course. So the researchers are in favour of short six-week courses of oxandrolone.
The study that is the subject of this article looks in more depth at the value of oxandrolone as a slimming aid. The men lost 1.8 kg fat during a 12-week course of oxandrolone, where the daily dose was 20 mg.
The table below shows how much of the fat had returned 12 weeks after the oxandrolone course had finished: less than 17 percent. That means that 83 percent of the weight lost stayed off.
So maybe oxandrolone has more potential as a diet drug than as a muscle builder, the researchers sigh [forgetting that a 2-kg fat loss over a 12 week period is perfectly possible without taking steroids].
 The more fat the men had lost, the lower their insulin level before a meal. This is a positive sign. A low pre-meal insulin level means that you are sensitive to insulin, and is associated with fewer inflammatory processes.
The more fat the men had lost, the lower their insulin level before a meal. This is a positive sign. A low pre-meal insulin level means that you are sensitive to insulin, and is associated with fewer inflammatory processes.
Ten years earlier endocrinologists discovered that a modest dose of oxandrolone reduces fat mass in men over 40, while men given a low dose of testosterone-enanthate build up more fat.
Oral anabolic steroid treatment, but not parenteral androgen treatment, decreases abdominal fat in obese, older men. Lovejoy et all 1995: These results suggest that SQ and visceral abdominal fat can be independently modulated by androgens and that at least some anabolic steroids are capable of influencing abdominal fat.”
And “Oral oxandrolone decreased SQ abdominal fat more than TE or weight loss alone and also tended to produce favorable changes in visceral fat.
”Neuroregenerative Effect of Oxandrolone - A Case Report Anabolic steroids have the clinical effect of increasing protein synthesis in muscle and other tissues. The brain and spinal cord neurons have gonadal steroid receptors and various studies have shown at structural and molecular levels that androgenic steroids have a significant trophic effect on the brain and spinal cord.
We evaluated the effect of Oxandrolone (an FDA-approved anabolic steroid) at the dose of 20 mg/day for 3 months added to concomitant exercise strength training 3 times a week in a patient affected by a demyelinating disease, Charcot-Marie-Toot 1 (CMT1). After the treatment, an increase in muscular strength and walking capacity was observed. Muscle biopsy revealed a significant increase of type grouping of muscle fibers, an expression of regeneration and reinnervation processes.
Data ensuing from this single case-report suggest that anabolic androgenic steroids have a potential neuroregenerative effect, with an inherent improvement in neuromuscular efficiency through an increased myelin synthesis at peripheral nervous system site.
Improved functional recovery after spinal cord injury. At present, only the corticosteroid, methylprednisolone, is used for acute spinal cord injury to improve function. However, improvements are modest, and are associated with myopathy and immunosuppression so that alternative treatments are needed. Oxandrolone is an androgenic steroid with potential neuroprotective properties that is used to prevent muscle loss and is not immunosuppressive. Oxandrolone increased locomotor recovery concomitant with reduced loss of cord tissue in a standard weight drop model of spinal cord contusion injury indicating oxandrolone as a possible alternative to methylprednisolone. Oxandrolone also increased axonal sprouting within the ventral horns distal to the injury consistent with formation of relay circuits mediating locomotor recovery.
