
Life Expectancy When On Steroids

Many iron warriors ask themselves if the use of anabolic steroids will shorten their lifespan. Or maybe prolong their lifespan. Is there any scientific research that could answer this question?
First if you ask someone this question, most people will first think of bodybuilders, because the (ab)use of anabolic androgenic steroids is inextricably linked to bodybuilders. Slowly the general population realizes that a big part of gymgoers and athletes uses AAS and not only for athletic purposes (doping) but also for cosmetic reasons. Is the use of anabolic steroids as dangerous as many officials want us to believe?
MEDICAL ISSUES ASSOCIATED WITH ANABOLIC STEROID USE: ARE THEY EXAGGERATED? Hoffman et all 2006: “Alterations in serum lipids, elevations in blood pressure and an increased risk of thrombosis are additional cardiovascular changes often associated with anabolic steroid use.
“Alterations in serum lipids, elevations in blood pressure and an increased risk of thrombosis are additional cardiovascular changes often associated with anabolic steroid use.
The magnitude of these effects may differ depending upon the type, duration, and volume of anabolic steroids used. Interesting to note is that these effects appear to be reversible upon cessation of the drug. In instances where the athlete remains on anabolic steroids for prolonged periods of time (e.g ”abuse”), the risk for developing cardiovascular disease may increase. Sader and colleagues (2001) noted that despite low HDL levels in bodybuilders, anabolic steroid use did not appear to cause significant vascular dysfunction.
Interestingly, athletes participating in power sports appear to have a higher incidence of cardiovascular dysfunction than other athletes, regardless of androgen use. Thus, a strength/power athlete with underlying cardiovascular abnormalities that begins using anabolic steroids is at a much higher risk for cardiovascular disease. However, anabolic steroid-induced changes in lipid profiles may not, per se, lead to significant cardiovascular dysfunction.”
D uring the sixties and seventies steroid use was not controlled, so wrestlers, power lifters, weight lifters and bodybuilders – if they wished – could legally inject and swallow as much as they wanted. Especially nandrolone (Deca) and Dianabol (Methandienone) where extremely popular. And although quite a few of them did just that, it had no effect on their life expectancy, researchers at the University of Gothenburg report in the Scandinavian Journal of Medicine & Science in Sports.
uring the sixties and seventies steroid use was not controlled, so wrestlers, power lifters, weight lifters and bodybuilders – if they wished – could legally inject and swallow as much as they wanted. Especially nandrolone (Deca) and Dianabol (Methandienone) where extremely popular. And although quite a few of them did just that, it had no effect on their life expectancy, researchers at the University of Gothenburg report in the Scandinavian Journal of Medicine & Science in Sports.
If you look at the bodybuilders from the “Golden Era”, like Franco Columbo, Arnold, Lou Ferrigno, Dave Draper, Frank Zane. All of them look better than 95% of the population of their age now. Sergio Oliva (July 4, 1941 – November 12, 2012
Nowadays there is such an enormous amount of money involved in elite sports, that almost everybody uses ergogenic means. The money also caused that elite athletes turned to medical specialists. In the USA the Balco scandal (Victor Conte) comes to mind. It ruined the careers of Marion Jones, Tim Montgomery and Barry Bonds, just to name a few. Dr Michele Ferrari (Tennis “Operation Puerto”), Dr. Luis Garcia del Moral (Lance Armstrong). In the year 2013, the judge refused to allow Dr. Fuentes to discuss names outside of cycling, such as footballers, athletes, cyclists, boxers and tennis players.
Elite bodybuilders that can afford it, hire “nutritonists” such as Chad or Charles.
Tour de France
Going by the amount of reports on doping use during the Tour de France, you'd expect that the competitors are more likely to have a shorter life span than the average population, but this study proved the opposite, French Tour de France riders live at least 6.3 years longer than the average French male.
A study presented at the European Society of Cardiology congress on Tuesday examined all 786 French competitors in the grueling bicycle race from 1947 to 2012. The researchers then compared the mortality rate among the cyclists with the mortality rate among the French male population. and found their death rate was 41 percent lower than average for French males.
The researchers divided 'their' cyclists into three groups. The first group was composed of cyclists that had competed during the period 1947 to 1970, when the most important doping substances used in the Tour de France were cocaine and amphetamines. The second group of cyclists competed in the period 1971-1990, when the main form of doping was anabolic steroids. The third group cycled between 1991 and 2012, the EPO and Growth Hormone era.
Riders in the Tour de France (which has been compared to running a marathon several days a week for nearly three weeks) actually had a 33 percent lower risk for death from heart attacks or strokes than the general population. The cyclists also died noticeably less from cancer [Neoplasms]
Powerlifters
I n 2000 epidemiologists at the Finnish National Public Health Institute published a very biased study, they wrote:
n 2000 epidemiologists at the Finnish National Public Health Institute published a very biased study, they wrote:
“Misuse of supraphysiological doses of anabolic steroids is claimed to have serious side effects. The aim of the study was to determine the mortality, and the cause of premature deaths among a group of subjects who are strongly suspected to have used anabolic steroids for a non-medical purpose over several years. The mortality of 62 male powerlifters placed 1st-5th in weight series 82.5-125 kg in Finnish championships during 1977-1982 was compared with the mortality of population controls.
They calculated that the mortality risk of elite power lifters was almost five times as high as that of the rest of the population.”
In 2014 in a retrospective 30-year follow-up study, Swedish researchers collected data on nearly 1200 athletes of former Swedish-elite male athletes in power sports
The aim of the study was to investigate mortality, including causes of death, in former Swedish male elite athletes, active 1960-1979, in wrestling, powerlifting, Olympic lifting, and the throwing events in track and field when the suspicion of former AAS use was high. R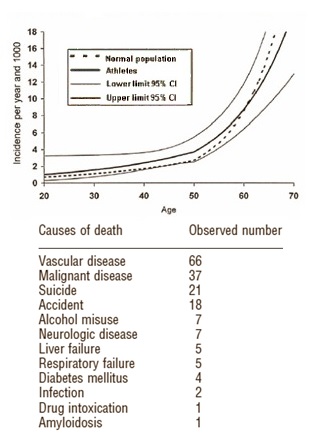 esults indicate that, during the age period of 20-50 years, there was an excess mortality of around 45%. However, when analyzing the total study period, the mortality was not increased.
esults indicate that, during the age period of 20-50 years, there was an excess mortality of around 45%. However, when analyzing the total study period, the mortality was not increased.
Mortality from suicide was increased 2-4 times among the former athletes during the period of 30-50 years of age compared with the general population of men.
"The death risk from suicide was 3.9 times higher for athletes than the normal population at the age of 30, 2.8 times higher at the age of 40 and 2.1 times higher at the age of 50."
Mortality rate from malignancy was lower among the athletes. The increased likelihood of suicide among the athletes is offset by a reduced chance of dying from cancer [Malignant disease]. The athletes were thirty percent less likely to die from cancer than the rest of the population. As a whole, the power athletes lived to the same age as the average Swede.
As the use of AAS was marked between 1960 and 1979 and was not doping-listed until 1975, it seems probable that the effect of AAS use might play a part in the observed increased mortality and suicide, all of whom did power sports during the sixties and seventies. The otherwise healthy lifestyle among the athletes might explain the low malignancy rates.
The same group of researchers came a year earlier (2013) to the conclusion: “It is clear that a relationship exists between use of AAS and mental-health problems. Further studies need to be done in order to clarify this relationship.”
Sudden or unnatural deaths involving anabolic-androgenic steroids.
I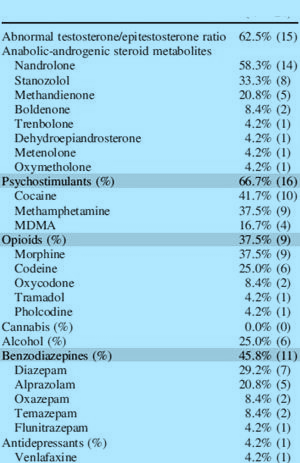 n 2014 the New South Wales Department of Forensic Medicine (Australia) wanted to determine causes of death, characteristics, toxicology, and pathology of AAS positive cases during 1995-2012. Only 24 cases could be linked to AAS use. All were male, and the mean age was 31.7 years. Deaths were mainly due to accidental drug toxicity (62.5%), then suicide (16.7%) and homicide (12.5%).
n 2014 the New South Wales Department of Forensic Medicine (Australia) wanted to determine causes of death, characteristics, toxicology, and pathology of AAS positive cases during 1995-2012. Only 24 cases could be linked to AAS use. All were male, and the mean age was 31.7 years. Deaths were mainly due to accidental drug toxicity (62.5%), then suicide (16.7%) and homicide (12.5%).
Abnormal testosterone/epitestosterone ratios were reported in 62.5%, followed by metabolites of nandrolone (58.3%), stanozolol (33.3%), and methandienone (20.8%).
In 23 of 24 cases, substances other than steroids were detected. Of the 24 deceased steroids users 23 were polydrug users. In addition to their steroids they had also used mainly stimulatory recreational drugs, but also sleeping pills and sedatives, opiates, alcohol and occasionally also antidepressants.
In nearly half, testicular atrophy was noted, as was testicular fibrosis and arrested spermatogenesis. Left ventricular hypertrophy was noted in 30.4%, and moderate to severe narrowing of the coronary arteries in 26.1%. To summarize, the typical case was a male polydrug user aged in their thirties, with death due to drug toxicity. Extensive cardiovascular disease was particularly notable.
