
How to protect joints, tendons and ligaments

If you want answers to this questions, you’ll find in all corners of the internet, the same article with high percentages of collagen increases by anabolic steroids. Many people copy and paste the same article sooner or later in almost every thread (posted below in blue). As with many online articles is difficult to find out who was the first one to post and like many articles this article doesn’t reveal its sources or the scientific studies that back up the claims.
What we see more often is that that some studies, like we always saw on older studies about anabolic androgenic steroids (AAS), that they just make claims about AAS, without making any differentiation about the kind of AAS, the application method, the doses etc.
Marqueti et al 2013: “We investigated the structural changes in the rat calcaneal tendon (CT), superficial flexor tendon (SFT), and deep flexor tendon (DFT) in response to jump exercises and anabolic androgenic steroids (AAS). In conclusion, exercise promoted benefits to the adaptation of the tendons to overload. These effects were absent when load exercise was combined with AAS. The abusive consumption of AAS contributes to tendon inertness and rigidity, and increases the potential risk of injury.” ..which kind of AAS at what doses and which timelength, if I may ask?
Not all anabolic androgenic steroids are equal.
The general consensus of the often cited article is true, the steroids that have more anabolic versus androgenic ratio like methenolone, oxandrolone, nandrolone etc. are beneficial for the tendons just like growth factors such as rhGH– IGF-1 etc. Also some trainings methods and behavioral factors prevent injuries and ruptures.
Fallanga et al reported that the anabolic steroid stanozolol stimulated overall collagen synthesis and increased the mRNA levels of a1(I) and a1(III) procollagen. These stimulatory effects of stanozolol on collagen synthesis were not observed with testosterone and were accompanied by increased synthesis of TGF-b1.
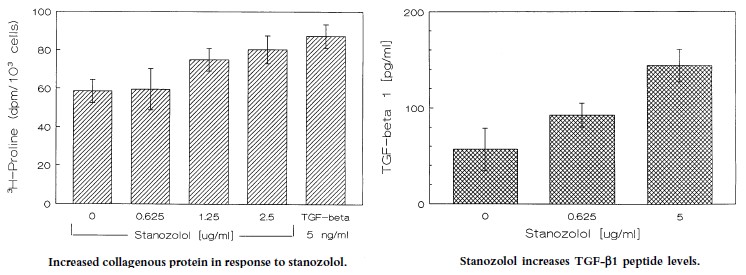
As seenin the representative experiment shown in the graphics above, stanozolol increasedcollagen synthesis by 35%. In the same experiment, higherconcentrations of stanozolol (1.25 and 2.5 mg per ml) were as effectivein stimulating collagen synthesis as TGF-b1 (5 ng per ml), which wasused here as an additional (positive) control. These results indicate that stanozolol increases overall collagenous protein synthesis. Total proteinreleased in the culture medium was not increased by stanozolol.
The mRNA levels of TGF-b1 were increased as early as 2 h after exposure of fibroblasts to stanozolol, and before any increase in procollagen mRNA. We found that stanozolol failed to stimulate collagen synthesis in TGF-b1 knockout fibroblasts and after the addition of a TGF- b1 anti-sense oligonucleotide and antibodies to TGF-b. Taken together, these findings strongly suggest that the stimulation of collagen synthesis by stanozolol is due, in large part, to the action of TGF-b1.
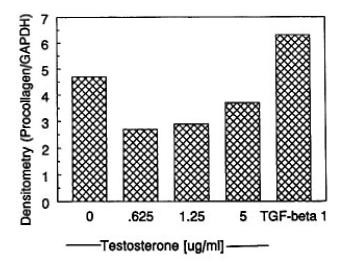 These stimulatory effects ofstanozolol on procollagen are most likely due to its anabolic rather than androgenic properties. Thus, as shown in the graphic left, similar molarconcentrations of testosterone (0.625–5mg per ml)failed to stimulate and actually decreaseda1(I) procollagen mRNA levels when compared with baseline measurements.
These stimulatory effects ofstanozolol on procollagen are most likely due to its anabolic rather than androgenic properties. Thus, as shown in the graphic left, similar molarconcentrations of testosterone (0.625–5mg per ml)failed to stimulate and actually decreaseda1(I) procollagen mRNA levels when compared with baseline measurements.
The stimulatory effects of stanozolol are due to TGF- b1. The action of stanozolol may be mediated by TGF-b1. TGF-b1 is a potent stimulus for collagen synthesis andits mRNA levels are increased by stanozolol.
 As shown, stanozolol increased TGF-b1 peptide levels by as much as 200%. Therefore, stanozolol increases both collagen and TGF-b1 synthesis. In fact, mRNA levels of TGF-b1 are increased as early as 2 h after exposure of fibroblasts to stanozolol, and before procollagen mRNA levels are increased. Although the increase (35%) in collagenous protein observed in this study may appear modest at first, it should be noted that the experiments were done in a defined serum-free media (AIM-V) without added growth factors, so as to avoid binding of stanozolol to steroid binding proteins. Moreover, the amount of collagen synthesis observed in response to stanozolol was the same as that measured after the addition of TGF-b1 and, importantly, the stimulatory actions of stanozolol appear to be specific, in that the parent compound testosterone actually decreased collagen synthesis.
As shown, stanozolol increased TGF-b1 peptide levels by as much as 200%. Therefore, stanozolol increases both collagen and TGF-b1 synthesis. In fact, mRNA levels of TGF-b1 are increased as early as 2 h after exposure of fibroblasts to stanozolol, and before procollagen mRNA levels are increased. Although the increase (35%) in collagenous protein observed in this study may appear modest at first, it should be noted that the experiments were done in a defined serum-free media (AIM-V) without added growth factors, so as to avoid binding of stanozolol to steroid binding proteins. Moreover, the amount of collagen synthesis observed in response to stanozolol was the same as that measured after the addition of TGF-b1 and, importantly, the stimulatory actions of stanozolol appear to be specific, in that the parent compound testosterone actually decreased collagen synthesis.
In animal studies, stanozolol has been reported to increase muscle protein synthesis without a directeffect on protein degradation. In vivo studies in humans have not specifically addressed the effects of anabolic steroids on extracellular matrix formation, but do point to overall anabolic activity. For example, a short-term study of 16 patients, eight of whom received 10mg of stanozolol rally each day for 14–21 d, showed an increase in the bulk of type I (oxidative) fibers in response to stanozolol. Other reports suggest that stanozolol may be effective in the treatment of osteoporosis, in improving nitrogen balance in wasting diseases such as muscular dystrophy, and in postoperative Trauma. Stanozolol has also been shown to cause dramatic healing of painful cutaneous ulcerations due to cryofibrinogenemia, however, it is unclear whether the beneficial effects of stanozolol in these dermal ischemic wounds is due to direct stimulation of tissue repair or to the fibrinolytic action of stanozolol.
Effect of high intensity aerobic exercise and mesterolone on remodeling of Achilles tendon of C57BL/6 transgenic mice Fontana et all 2010:
 “The effect of mesterolone and intensive treadmill training (6 weeks, 5 days/week, means: 15.82 m/min and 45.8 min/day) in Achilles tendon remodeling was evaluated. Sedentary mice treated with mesterolone or vehicle (placebo) and corresponding exercised (with mesterolone and without) were examined.”
“The effect of mesterolone and intensive treadmill training (6 weeks, 5 days/week, means: 15.82 m/min and 45.8 min/day) in Achilles tendon remodeling was evaluated. Sedentary mice treated with mesterolone or vehicle (placebo) and corresponding exercised (with mesterolone and without) were examined.”
Conclusion: “Thus, mechanical stimuli and mesterolone alter the morphology of tenocytes and the composition of the tendon, probably through fibrillogenesis and/or increased intermolecular cross-links. The ergogenic effect is evidenced by the activation of collagenous and non-collagenous protein synthesis and the increase in the diameter and area of collagen fibrils. This study might be relevant to clinical sports medicine.”
 Nandrolone Decanoate (DecaDurabolin aka DECA) Nandrolone Decanoate has an enormous lot of scientific research to back up its use in athletes, power athletes and as a drug for medical applications.
Nandrolone Decanoate (DecaDurabolin aka DECA) Nandrolone Decanoate has an enormous lot of scientific research to back up its use in athletes, power athletes and as a drug for medical applications.
Back in 1983, the FDA approved NandroloneDecanoate for treating osteoporosis; so it should be no surprise that Deca increases bone density. The body itself produces nandrolone in tiny quantities, possibly to aid the repair of damaged soft tissue. Thus the use for exogenous administration of higher doses of nandrolone is obvious.
Joint pain is pretty common in people as they age and/or in bodybuilders who engage in intense workouts. It should be little surprise that the latter group really appreciates the positive Deca Durabolin effects on joint paint. Research has shown that even when dosed at 50mg once every three weeks, Nandrolonedecanoate can stimulate type III collagen synthesis in joints. The drug also boosted both intestinal calcium absorption and bone mineral content. So at higher doses, it's easy to understand how bodybuilders and powerlifters with joint pain suddenly feel better after running a deca cycle.
 Nandrolone also can increase hemoglobin and red blood cell mass, making it popular with endurance athletes. The list of athletes banned for the use of nandrolone is endless. Nowadays many athletes also use shorter acting nandrolones, which have shorter clearance times and thus reduces the chance to be detected in a doping test. For non-doping reasons DecaDurabolin – NPP or a combination can be used according to the goals of the user.
Nandrolone also can increase hemoglobin and red blood cell mass, making it popular with endurance athletes. The list of athletes banned for the use of nandrolone is endless. Nowadays many athletes also use shorter acting nandrolones, which have shorter clearance times and thus reduces the chance to be detected in a doping test. For non-doping reasons DecaDurabolin – NPP or a combination can be used according to the goals of the user.
Decenaet al 2010 on Nandrolone Phenylpropionate in veterinary research:
“Steroids have long been used for different purposes including both aesthetic and therapeutic reasons. In animals steroids have been used for pain, inflammation and allergy but they were also used for fattening up, achieving volume and building muscle mass. Since steroids are known to increase muscle mass in animals, it is not uncommon for animals to be injected with anabolic steroids.
The steroid used in this experiment was Nandrolone Phenylpropionate under the brand name of Slazbolak. This steroid is a Nandrolone-derived progestin produced by removing the carbon atom at the 19th position of the Steran Nucleus of testosterone. Some of its beneficial effects include improvement of collagen synthesis and bone mineral content, anti-inflammatory response and catabolic reversion. It has an anabolic/androgenic miceio of 125:37, making it highly anabolic and modemiceely androgenic. Nandrolone converts only a fifth of the testosterone to estrogen when it interacts with the aromatase enzyme significantly lessening the problem of side-effects related to feminine features.
This steroid is popular among human males because the above mentioned characteristics of Nandrolone already edges out other steroids that have significantly more risks of side effects.
Even though Nandrolone Phenylpropionate is similar to the popular steroid of NandroloneDecanoate (which has a longer ester), NandrolonePhenylpropionate is shorter acting meant for practical intents and purposes and produce less water retention and is consistent with other injectable testosterones. Nandrolone has the ability to improve collagen synthesis and bone mineral content, benefitting joints and connective tissues. Hence, nandrolone steroids would be detected better via bone structure observation.
Finally, the hearts of all the animals yielded an increase in gross weight. Steroids are known to cause cardiac hypertrophy and the results are indeed in line with this but it still does not eliminate other possibilities".
Ego
 All anabolic steroids (AAS) can cause injuries and tendon ruptures, because muscle mass and strength develop faster, than ligaments and tendons develop and strengthen. It is therefore wise totrain heavy and intense BEFORE you start to cycle AAS. The steroids also increase aggression and that will increase your lust to train, and to train heavier and longer. Steroids will also reduce fatigue and mask pain, that again can cause overtraining and thus inflammation, injury or rupture. I’ve seen many guys that with increasing muscle mass showed increased ego and felt the necessity to show how heavy they could lift.
All anabolic steroids (AAS) can cause injuries and tendon ruptures, because muscle mass and strength develop faster, than ligaments and tendons develop and strengthen. It is therefore wise totrain heavy and intense BEFORE you start to cycle AAS. The steroids also increase aggression and that will increase your lust to train, and to train heavier and longer. Steroids will also reduce fatigue and mask pain, that again can cause overtraining and thus inflammation, injury or rupture. I’ve seen many guys that with increasing muscle mass showed increased ego and felt the necessity to show how heavy they could lift.
The Power of Partials
Powerlifters have long been using partial movement exercises to bust through plateaus and strengthen joints and tendons. By only performing around ¼ of the full range of movement (ROM) on power lifts, lifters are able to use much heavier weights than usual – somewhere in the 120-130% one rep max range.
This is primarily used to strengthen tendons and other connective tissues, but it also puts huge loads on the muscles, resulting in significant strength and mass gains.
It isalso worth mentioning the elephant in the room of strength sports, too:steroid use. Because muscles grow much, much faster than tendons when on steroids, many steroid users frequently bust their joints whilst on cycles. Partial training is essential for steroid users to strengthen and thicken their tendons.
The extra load you’ll be lifting with partials can also “shock” your muscles into hypertrophy and add kilograms to your normal lifts, which in turn will result in lean mass gains.
By incorporating this into your normal bodybuilding training, you can diversify your training, reduce the risk of injury and become much, much stronger – resulting in a more symmetrical, thicker physique. Best of all, learning from other iron sports, be that strongman, Olympic lifting or powerlifting can give bodybuilders a whole new perspective on training and strength.
From mechanical loading to collagen synthesis, structural changes and function in human tendon. Kjaer et al 2009
 The adaptive response of connective tissue to loading requires increased synthesis and turnover of matrix proteins, with special emphasis on collagen. Collagen formation and degradation in the tendon increases with both acute and chronic loading, and data suggest that a gender difference exists, in that females respond less than males with regard to an increase in collagen formation after exercise. It is suggested that estrogen may contribute toward a diminished collagen synthesis response in females. Conversely, the stimulation of collagen synthesis by other growth factors can be shown in both animal and human models where insulin-like growth factor 1 (IGF-I) and transforming growth factor-beta-1 (TGF-beta-1) expression increases to accompany or precede an increase in procollagen expression and collagen synthesis. In humans, it can be demonstrated that an increase in the interstitial concentration of TGF-beta, PGE2, IGF-I plus its binding proteins and interleukin-6 takes place after exercise. The increase in IGF-I expression in tendon includes the isoform that has so far been thought only to exist in skeletal muscle (mechano growth factor). The increase in IGF-I and procollagen expression showed a similar response whether the tendon was stimulated by concentric, isometric or eccentric muscle contraction, suggesting that strain rather that stress/torque determines the collagen-synthesis stimulating response seen with exercise.
The adaptive response of connective tissue to loading requires increased synthesis and turnover of matrix proteins, with special emphasis on collagen. Collagen formation and degradation in the tendon increases with both acute and chronic loading, and data suggest that a gender difference exists, in that females respond less than males with regard to an increase in collagen formation after exercise. It is suggested that estrogen may contribute toward a diminished collagen synthesis response in females. Conversely, the stimulation of collagen synthesis by other growth factors can be shown in both animal and human models where insulin-like growth factor 1 (IGF-I) and transforming growth factor-beta-1 (TGF-beta-1) expression increases to accompany or precede an increase in procollagen expression and collagen synthesis. In humans, it can be demonstrated that an increase in the interstitial concentration of TGF-beta, PGE2, IGF-I plus its binding proteins and interleukin-6 takes place after exercise. The increase in IGF-I expression in tendon includes the isoform that has so far been thought only to exist in skeletal muscle (mechano growth factor). The increase in IGF-I and procollagen expression showed a similar response whether the tendon was stimulated by concentric, isometric or eccentric muscle contraction, suggesting that strain rather that stress/torque determines the collagen-synthesis stimulating response seen with exercise.
Feed Your Joints
 Supplementation and nailing micronutrient intake is also an important part of recovery. Bodybuilders will always have their macro-nutrient intake nailed, but many neglect their intake of essential vitamins and micronutrients.Glucosamine and chondroitin have been medically shown to help tendons and connective tissues repair, and when combined with MSM, magnesium and vitamin C, will give your joints the boost they need to keep up with your training.
Supplementation and nailing micronutrient intake is also an important part of recovery. Bodybuilders will always have their macro-nutrient intake nailed, but many neglect their intake of essential vitamins and micronutrients.Glucosamine and chondroitin have been medically shown to help tendons and connective tissues repair, and when combined with MSM, magnesium and vitamin C, will give your joints the boost they need to keep up with your training.
The most effective dosages reported in the medical research studies is 1,500 mg Glucosamine and 1,200 mg Chondroitin sulfate per day. Make sure that whichever product you buy gives you these dosages, spread out over 2 to 3 pills daily. Personally, I recommend the 3-in-1 glucosamine, chondroitin and MSM pill from TGF-b1 is an established stimulus for the formation of extracellular matrix both in vitro and in vivo. The results shown here point to TGF-b1 being critically involved in the stimulatory action of anabolic steroids on collagen synthesis.
This observation is of interest when one considers the possibility of using anabolic steroids to offset the deleterious effects of corticosteroids on wound healing. For example, in one study of experimental cutaneous wounds in rats, it was shown that the systemic administration of TGF-b1 reversed the inhibitory effects of corticosteroids on healing. In another report of anastomotic healing of intestinal wounds, stanozolol reversed the inhibition of healing caused by corticosteroids. Therefore, it is plausible that TGF-b1 plays an important role in the way anabolic steroids work, or at least in the way they oppose some of the effects of corticosteroids.
 In conclusion, we provide evidence that stanozolol stimulates collagen synthesis. If these effects are mediated through TGF-b1, as our results indicate, we should start thinking of anabolic steroids as acting pharmacologically to increase the synthesis of potent growth factors and cytokines.
In conclusion, we provide evidence that stanozolol stimulates collagen synthesis. If these effects are mediated through TGF-b1, as our results indicate, we should start thinking of anabolic steroids as acting pharmacologically to increase the synthesis of potent growth factors and cytokines.
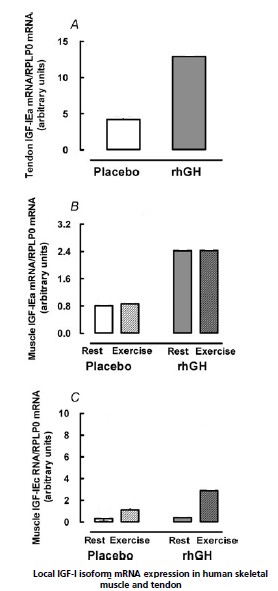
Growth hormone stimulates the collagen synthesis in human tendon and skeletal muscle without affecting my ofibrillar protein synthesis. Doessing et al 2009
In skeletal muscle and tendon the extracellular matrix confers important tensile properties andis crucially important for tissue regeneration after injury. Musculoskeletal tissue adaptation is influenced bymechanical loading, whichmodulates the availability of growth factors, including growth hormone(GH)and insulin-like growth factor-I (IGF- I),whichmay be of key importance.
To test the hypothesis that GH promotes matrix collagen synthesis in musculotendinous tissue, we investigated the effects of 14 day administration of 33–50 μg kg−1 day−1 recombinant human GH (rhGH) in healthy young individuals. rhGH administration caused an increase in serum GH, serum IGF-I, and IGF-I mRNA expression in tendon and muscle. Tendon collagen I mRNA expression and tendon collagen protein synthesis increased by 3.9-fold and 1.3-fold, respectively, and muscle collagen I mRNA expression and muscle collagen proteinsynthesis increased by 2.3-fold and 5.8-fold, respectively. Myofibrillarprotein synthesis was unaffected by elevation of GH and IGF-I. Moderate exercise did not enhance the effects of GH manipulation. Thus, increased GH availability stimulates matrix collagen synthesis in skeletal muscle and tendon, but without any effect upon myofibrillarprotein synthesis. The results suggest that GH is more important in strengthening the matrix tissue than for muscle cell hypertrophy in adult human musculotendinous tissue.
Oxandrolone
 Saggerset all : “In vivo, there are reported increases in wound breaking strength with anabolic steroid therapy, including oxandrolone. During the early stages of gain in wound breaking strength of healing incisional wounds, there is increased deposition of new collagen. These studies support the notion that oxandrolone enhances the deposition of collagen in wounds by directly increasing the expression of both type III and type I procollagen mRNA. The relevance of these observations to the clinical setting may be described by the following scenario. Oxandrolone has been shown to facilitate weight gain in patients with weight loss and pressure ulcers. Oxandrolone increases nitrogen retention, enhancing proteinsynthesis. As weight is restored and protein reserves are depleted, wound closure ensues. Along with this systemic response, evidence is mounting for a possible direct effect of oxandrolone on wounds. This is shown by the increased collagen cellularity and tensile strength described in vivo, the mechanism of which may be the increased expression of collagen on the cellular level, presented here.”
Saggerset all : “In vivo, there are reported increases in wound breaking strength with anabolic steroid therapy, including oxandrolone. During the early stages of gain in wound breaking strength of healing incisional wounds, there is increased deposition of new collagen. These studies support the notion that oxandrolone enhances the deposition of collagen in wounds by directly increasing the expression of both type III and type I procollagen mRNA. The relevance of these observations to the clinical setting may be described by the following scenario. Oxandrolone has been shown to facilitate weight gain in patients with weight loss and pressure ulcers. Oxandrolone increases nitrogen retention, enhancing proteinsynthesis. As weight is restored and protein reserves are depleted, wound closure ensues. Along with this systemic response, evidence is mounting for a possible direct effect of oxandrolone on wounds. This is shown by the increased collagen cellularity and tensile strength described in vivo, the mechanism of which may be the increased expression of collagen on the cellular level, presented here.”
To summarise
Bodybuilders, powerlifters and other iron adepts share their experiences with each other for decades. And yes, sometimes bro-science and articles that contain made-up percentages are posted. But in broad lines the story is true, AAS with a more anabolic to androgenic ratio are better in preserving healthy joints, ligaments and tendons. What we often do and what seldom shows up in scientifical research is the combination of anabolic steroids that enhance each other’s quality, what we call synergy. Roids are also combined with peptides for an even better result. rhGH(somatropine) has become normal and combined with nandrolone or boldenone and oxandrolone is an excellent cycle for athletes that go through injury or just sore joints. Combine it with high end supplements containing Glucosamine and Chondroitin and you will be fine.
From adiscussion board: “Low dose Deca blended with Equipoise........... BOOOOM........... Joints feel like they have been axle greased.”
