
Growth Hormone Usage and History

 When in the early eighties of the last century it became known that recombinant HGH would become available on the market, the expectations of athletes were high. Dan Duchaine had in his book Underground Steroids written an attractive description of the progress that could be achieved with recombinant human growth hormone (rhGH). No steroids were able to match that. This was also pretty much the general belief. Understandably, the release of the biosynthetic form of this hormone was eagerly awaited.
When in the early eighties of the last century it became known that recombinant HGH would become available on the market, the expectations of athletes were high. Dan Duchaine had in his book Underground Steroids written an attractive description of the progress that could be achieved with recombinant human growth hormone (rhGH). No steroids were able to match that. This was also pretty much the general belief. Understandably, the release of the biosynthetic form of this hormone was eagerly awaited.
Ok, human growth hormone was already circulating on the [black] market, but that was hGH from the pituitary glands of deceased donors, also called cadaveric hGH. Now the real, identical biosynthetic growth hormone would be made available. Although the donor hGH is also identical, it has to be of course, but from the new recombinant product was expected a lot more.
 Like so many times: when the expectations are high, the reality is often disappointing. First rhGH was expensive, very expensive and therefore only affordable for a small minority of athletes. For a small cycle of rhGH you paid 400-700 dollars per week. Partly because it was so expensive, the used dosages where too low to meet the high expectations. There was some progress, but much less than avid users had initially hoped for. It soon became clear that GH alone, had no spectacular results to offer to the athlete under 40 years.
Like so many times: when the expectations are high, the reality is often disappointing. First rhGH was expensive, very expensive and therefore only affordable for a small minority of athletes. For a small cycle of rhGH you paid 400-700 dollars per week. Partly because it was so expensive, the used dosages where too low to meet the high expectations. There was some progress, but much less than avid users had initially hoped for. It soon became clear that GH alone, had no spectacular results to offer to the athlete under 40 years.
The situation became different when AAS had also been added to the cycle, and even better if also around 25 mcg thyroxine [T4] every other day (EOD) was taken also. Lean mass gain during a “bulk phase” was higher than with AAS alone and ... very important: the loss during the “off period” was limited. With an AAS alone cycle , after stopping two thirds of the gains in mass and strength should be retained. At least when the training was modified to the reduced growth capacity of the body, and a good PCT was used. When GH was included in the cycle than was the loss of mass was limited to about 10-20% . Ergo, someone who during a cycle of AAS and GH in 6 weeks, gained 12 pounds will with a well-dosed training load, will loose on average 0.6 to 1.2 kg, with AAS alone that is in the most favorable case 2 kg. This preservation is probably partly due to increased bone mass. Off course most of these figures are hypothetical and highly individual and case (AAS dose) depended
GH synergy with Testosterone
A study from Meinhardt et al (2010), showed that in healthy adult men and women who exercise recreationally, GH (6 IU/day) significantly increased Wingate sprint performance— a measure of anaerobic power— by 4 percent compared to a control group that was not treated. Men experienced a synergistic increase in the Wingate test to 8.3 percent when testosterone was also administered (250 mgs Sustanon/week) along with GH. Interestingly, while testosterone and GH both increased lean mass, GH did so by increasing extracellular water; testosterone actually increased muscle tissue.
Before we come to the how and why, I will first give a brief history of growth hormone.
History
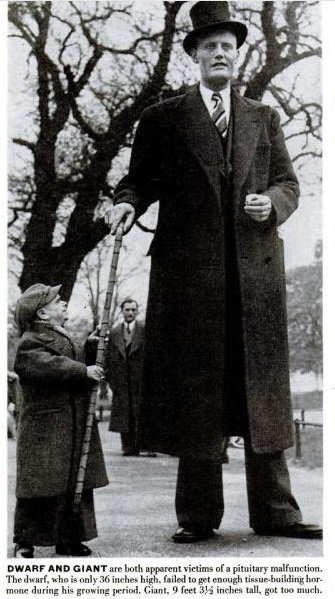
The name 'Growth Hormone' was chosen because the absence of this compound (hormone) caused a slow pace and finally stopped the [length] growth of the body. The first and most visional effect of STH. History is full of stories, drawings and photos of “midgets” and “dwarfs”. Unlike the so-called. "Lilliputians”, these are adults with growth hormone deficiency in their childhood and perfectly in proportion. Only small, between 120 and 150 cm. Nowadays, now we better understand the how and why, we prefer to call them “small people” which in fact is what they are.
 I will not discuss the various forms of GH deficiency / insufficiency here, that would take us beyond the scope of this review article. It has lasted until the middle of the 20th century before endocrinologists fully understood the implications of growth hormone deficiency. Then a curing drug had to be found.
I will not discuss the various forms of GH deficiency / insufficiency here, that would take us beyond the scope of this review article. It has lasted until the middle of the 20th century before endocrinologists fully understood the implications of growth hormone deficiency. Then a curing drug had to be found.
Since 1920’s from the pancreas of cows and swine’s we already harvested another peptide hormone: insulin. Insulin could be used to treat diabetes patients. A breakthrough.
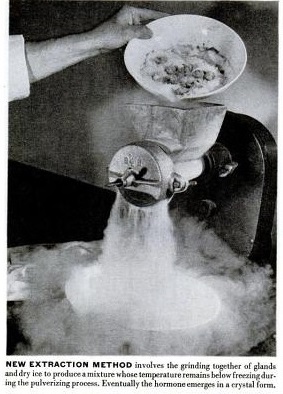
Unfortunately, experiments with pig and cattle-GH in children with GH deficiency yielded disappointing results. GH proved to be highly species-specific, that means only human growth hormone provides effects in humans. Non species-specific GH, like bovine or pig GH, could provide allergic reactions, or even an anaphylactic shock in humans. In the late 1940’s the endocrinologist Maurice Raben managed to isolate enough GH from the pituitary glands of human cadavers to treat a boy with GH deficiency successfully. A major breakthrough!
Endocrinologists, who had focused on the treatment of children, where approaching pathologists with the request of harvesting human pituitary glands during autopsies. These were [mostly by the parents of GH deficient children themselves] given to chemists to produce enough purified GH for their children. It will be clear that only a fraction of the children who needed this treatment with GH, where able to get it. That was not fair and the government did everything possible to provide therapy for more [if possible all] patients with severe GH. I sketch here mainly the developments in the USA, but in Western European countries similar processes took place. In 1960, the NPA [National Pituitary Agency] was established as a separate unit within the US Institute of National Health. The NPA systematized harvesting pituitaries, as well as the isolation of GH. The resulting drug, donor-GH, was all made available to endocrinologists who specialized in treating children. The supply of this "cadaver GH" was extremely limited, so only the most severe patients could be helped. Meanwhile, [1976] it was found out that donor-GH could convey Creutzfeldt Jacob disease [the human variant of the mad cow disease].
 In 1977, everything was being done to perfect the refining of Cadaver GH. Unfortunately, the number of autopsies, in which pituitary glands were obtained decreased significantly in that time. At the same time the number of patients grew [not the patients themselves] Due to the scarcity and strictly controlled distribution of human GH, treatment was usually discontinued when the children had reached an 'acceptable length'. That limit was just over 1,50 meter! Late seventies last century, the Swedish pharmaceutical factory Kabi Vitrum released the first commercial GH market “Crescormon” was the brand name. This gave, what else, conflicts with the NPA. In the first place because the NPA feared that Kabi would buy pituitaries in the US and thus reducing the stock of the NPA. But they were also fearful of a global trend in which pituitary glands were sold to those who were willing to pay the most for it. Further they strongly disapproved that Kabi aimed their campaign at general practitioners, the "first line" health care. Endocrinologists specialized In work with GH deficient children felt hereby excluded. Meanwhile, the black market in Europe and the US was flooded with hormones from the former Soviet Union. As in the SU no permission was sought from the family, and with each standard autopsy the pituitary was removed. The powder looked a filthy-grey, not especially an inviting little substance. Nevertheless, there was a growing demand in the athletic/bodybuilding world to what looked like cigarette ash, more than a carefully manufactured drug.
In 1977, everything was being done to perfect the refining of Cadaver GH. Unfortunately, the number of autopsies, in which pituitary glands were obtained decreased significantly in that time. At the same time the number of patients grew [not the patients themselves] Due to the scarcity and strictly controlled distribution of human GH, treatment was usually discontinued when the children had reached an 'acceptable length'. That limit was just over 1,50 meter! Late seventies last century, the Swedish pharmaceutical factory Kabi Vitrum released the first commercial GH market “Crescormon” was the brand name. This gave, what else, conflicts with the NPA. In the first place because the NPA feared that Kabi would buy pituitaries in the US and thus reducing the stock of the NPA. But they were also fearful of a global trend in which pituitary glands were sold to those who were willing to pay the most for it. Further they strongly disapproved that Kabi aimed their campaign at general practitioners, the "first line" health care. Endocrinologists specialized In work with GH deficient children felt hereby excluded. Meanwhile, the black market in Europe and the US was flooded with hormones from the former Soviet Union. As in the SU no permission was sought from the family, and with each standard autopsy the pituitary was removed. The powder looked a filthy-grey, not especially an inviting little substance. Nevertheless, there was a growing demand in the athletic/bodybuilding world to what looked like cigarette ash, more than a carefully manufactured drug.
Synthetic HGH
In 1981 the new company Genentech started in collaboration with Kabi the development and testing of bio synthetic human growth hormone. The drug was obtained by 'building-in' human genes in bacteria. Soon reaction-vessels were full of bacteria almost continuously producing the peptide hormone. It was a new drug and the period of effectiveness and safety testing before it could come to the market, was stretched to almost four years. But then it was there: Protropin®. A period of severe GH scarcity came to an end and there were in principle no more obstacle for mass production, the launch price was to say the least on the high side. In the US, the cost of treating GH deficient children somewhere between ten and thirty thousand dollars a year! The competition was not sleeping and therefore it did not take long before other pharmaceutical giants released their own recombinant STH on the market. Eli Lilly [Humatrope®] Pharmacia [formerly Kabi Vitrum and now Pfizer] [Genotropin®] Serono [Saizen®] Pharmacia and Novo Nordisk [Norditropin®] Genentech came with  Nutropin® Teva with Tev-tropin®. The prices were not very different and just remained high.
Nutropin® Teva with Tev-tropin®. The prices were not very different and just remained high.
All these brands of recombinant HGH not only provided a safe source of HGH for kids with growth disorders, but the increase in supply of HGH meant experimentation with other applications for the hormone. One was the explosion of black-market HGH use by athletes to improve their performance. In 1986, The Washington Post reported some doctors predicting that use of HGH in athletes "could lead to the day that, instead of cheering for 'The Fridge' [nickname of 6'2" 380-pound, fan favorite William Perry, a player for the Chicago Bears in the mid-1980s], fans would be yelling for three-bedroom colonials." Though house-sized athletes never materialized, HGH continued to be a favorite drug for doping, particularly because it was difficult to detect in tests. Recent improvements in testing, however, may soon change HGH's place in sports. April of 2012 marked the first time that a U.S. athlete (weightlifter Pat Mendes) was banned from the Olympic Games for a positive test for HGH.
 Good times
Good times
In the late 1990′s and early to mid-2000′s it was very easy to find and buy high quality growth hormone online without a prescription. In the west (USA, Canada, EU, Australia) it was perfectly legal to buy almost any medicine for personal use. It was ok to import medicine from Asia as long as it was not classified as a narcotic and the quantity did not exceed what an average person would use within 3 months’ time. There were no low quality brands on the market because high quality HGH was readily available. There was an occasional counterfeit copy but that problem was easily solved by introducing verifiable authenticity stickers on the original HGH boxes.
Between 1997 to 2007 the Chinese growth hormone brand Jintropin® rose to popularity to the point it rivaled western big pharma HGH brands on their own home markets. Jintropin was by far the most widely used HGH for non-medical use. People used it freely for anti-aging, fat loss, bodybuilding, general well-being, etc. The manufacturer (GeneScience) was not shy to advertise it as such.
Bad times
As western “big pharma” is one of the strongest pillars of “world power” they have their ways of getting things done (influencing politics, etc). As western markets are the only place where they can overprice a product by tenfold and get away with it – it is the only area worth conquering and dominating by any means necessary. To be able to dominate medicine sales on the western markets, they needed to remove the 10 times cheaper Asian competition. This is how it was done: Plan A was to do it the same way any other industry goes at cheaper Asian products – stereotyping them as low quality and/or dangerous. This didn’t work for growth hormone because users were encouraged to have Jintropin lab tested (and they did). They were able to personally compare the results between Chinese HGH and western big pharma brands. Jintropin’s reputation grew regardless of what was thrown at it.
Even Sylvester Stallone was caught importing it into Australia for his own use, which was a huge story back then.
Plan B came in 3 phases. First the “big media” propaganda industry was unleashed with the objective to demonize human growth hormone as a dangerous substance and importing from Asia as very bad in every way imaginable. During that period I had set my google news alerts to receive daily news digest on HGH related topics. Almost every day another sport celebrity was caught using HGH. Celebrity names were used to draw attention to the stories, which then went on to describing how horrible and dangerous the growth hormone is and how something should be done to stop it.
After demonization it was time for phase 2, which was to make HGH illegal to import. In 2007 growth hormone was classified to be in the same group as anabolic steroids and made illegal to buy without a prescription or sell without a license. Who can obtain a license in the western markets? Only western manufacturers, local pharmacies and local doctors. Local doctors are unable to prescribe non FDA approved (any Asian) medicine while local pharmacies are not allowed to sell non FDA approved (any Asian) HGH. Thus the groundwork was successfully laid – after 2007 only western big pharma HGH brands were allowed to be sold in the western markets.
The rules changed overnight which made the non-western based manufacturers and sellers of growth hormone (whose livelihood depended on the sales) illegal.
Thus came the time for phase 3, which was to go after the now “rogue” sellers and manufacturers. In case of Jintropin manufacturer (Gensci) – one day they were good guys for providing high quality product at tenfold lower prices as compared to the big pharma made HGH, the next day their CEO was portrayed in the media as a “drug cartel kingpin” and wanted for trial in USA.
What happened after that is just my educated guess (I have nothing to do with Gensci). The trial for the CEO never happened but some serious politics seemed to be involved. Gensci briefly lost the license in China to produce Jintropin, some of their money was frozen and possibly “confiscated” or used to pay whoever needed to be paid to let things go. After that, their license was restored, everything was back to normal with one difference – they stopped selling to the western markets.
As the only lab in China capable of producing the highest quality HGH at the time, Gensci’s Jintropin represented 80% of the Chinese HGH market sales. The remaining 20% went to the medium grade Ansomone by Ankebio and a few other small manufacturers capable of producing lower grade somatropin.
Aftermath
The HGH vacuum left on the western markets was soon filled by countless new brands. Some of them may or may not be produced by Gensci’s know-how, equipment and procedure ( Hygetropin). The vast majority of the now considered “black market” HGH brands which are available today are either counterfeit or low quality “generic HGH” named and branded as the customer/reseller wants (Riptropin, Kigtropin, Getropin, Taitropin, Glotropin, whatever-you-can-think-of-tropin). Some of these brands are made to look as if they are produced in USA or Europe (Europharma, Eurobolic, Euro-whatever). They are even shipped from EU by whoever previously imported them from Asia at wholesale quantities.
The small manufacturers (mostly Chinese, some Indian) seem to have benefited from the illegalization of Asian HGH the most. With the “giant” Gensci barred from selling, the small-timers got a chance to establish themselves. As they are underground labs, their manufacturing practices and techniques are unknown. Chances of them being able to obtain the required multi-million dollar equipment and skilled people necessary to produce proper high quality somatropin are slim. They are able to offer their products at a fraction of the price when compared to the high quality HGH. The low price makes these brands attractive to the resellers, who push them onto end buyers, who are then disappointed by the results and learn to stay away from HGH in the future. I run into an occasional horror story of painful red welts around injection spots, infections, raised HGH antibodies, etc.
Even though there has been no shortage of high quality Hygetropin on the market since 2007 and in the recent years Gensci seems to be recovering by establishing Jintropin legally in Russia, Mexico and some other “third world” countries from where it is apparently being sold to the western black markets again, the damage to the image of “Chinese HGH” might be difficult to repair. New users initially run into any of the low quality brands because they are more affordable. Bad experience then equals more bad reviews for “Chinese HGH”.
Furthermore the big pharma industry with all its extensions (FDA, legitscript, etc) is still aggressively pursuing online sellers of growth hormone. They even go as far as to force the western domain registrars to confiscate the domains of what they consider to be “rogue pharmacies”. This is effectively any seller not licensed by their attack dog – legitscript.com. It feels as if they own the internet and the rest of the world doesn’t matter. Why? Because they can.
EthicsWhen GH was still extremely scarce, could you could rightly claim that the use of this hormone for sports purposes was unethical. Once it was produced almost “en masse”, that argument falls away. Nevertheless, ethical questions remain to medical restrictions. The vast majority of doctors will still find administration to healthy athletes unethically. And yes, what about parents who come to a doctor and ask: '' My son is fourteen and wants to become a basketball player, can you prescribe GH"? When the boy would reach a normal length and is not GH deficient, very few physicians will be found who are inclined to for fill this request. And what about the people who want to lose weight, is using rhGH ethical for that reason. Obesity is a health problem of the first order and especially abdominal fat accumulation. Men with advancing years show increasingly more belly fat which increases the risk of heart disease and type 2 diabetes.
become a basketball player, can you prescribe GH"? When the boy would reach a normal length and is not GH deficient, very few physicians will be found who are inclined to for fill this request. And what about the people who want to lose weight, is using rhGH ethical for that reason. Obesity is a health problem of the first order and especially abdominal fat accumulation. Men with advancing years show increasingly more belly fat which increases the risk of heart disease and type 2 diabetes.
For now, the slimming is no indication for rhGH therapy, unless patients are in the group GH deficient adults. One of the most striking effects of GH is that it promotes the fatty acid oxidation. Especially visceral fat [located in the abdominal cavity] is reduced in fairly rapid pace. Already noticeable in the first weeks of medication.. As an adjunct to a weight loss program, I think usage of rhGH is certainly ethical. Even if not always reliable, IGF1 level remain within the 'normal' limits.
Recombinant HGH not only provided a safe source of HGH for kids with growth disorders, but the increase in supply of HGH meant experimentation with other applications for the hormone. One was the explosion of blackmarket HGH use by athletes to improve their performance. In 1986, The Washington Post reported some doctors predicting that use of HGH in athletes "could lead to the day that, instead of cheering for 'The Fridge' [nickname of 6'2" 380-pound, fan favorite William Perry, a player for the Chicago Bears in the mid-1980s], fans would be yelling for three-bedroom colonials." Though house-sized athletes never materialized, HGH continued to be a favorite drug for doping, particularly because it was difficult to detect in tests. Recent improvements in testing, however, may soon change HGH's place in sports. April of 2012 marked the first time that a U.S. athlete (weightlifter Pat Mendes) was banned from the Olympic Games for a positive test for HGH.
IndicationsThe purpose of rhGH medication, can be roughly divided into three areas. Beware, this overlaps, but the division makes the whole GH usage a little clearer. We distinguish: MEP [Medical Purposes], PEP [Performance Enhancement Purposes] and LEP [Life Extension Purposes], life extension needs to be taken here is very spacious. It's not just about the number of years we live, but especially for the quality of life, according to some doctors, GH is for this purpose almost a panacea. It is impossible to prescribe a standard dose for all areas.
MEP
Includes: GH deficiency in children, Turner- and Prader Willi syndrome, chronic kidney disease, stunted growth of the fetus in the womb and HIV / AIDS. GH does not cure these diseases, but may improve the quality of life for the patient significantly. Furthermore, it is used to promote recovery after major surgery and [often locally] applied to burns. Not with open heart surgeries and in patients on Intensive Care. Here, the number of death increases due to yet unknown causes, when rhGH is administered.
And then there is another important indicator of GH deficiency in adults. This deficiency leads to early aging, degeneration of bones, obesity, type 2 diabetes and a number of other symptoms of deterioration. It remains difficult to determine who is GH deficient. Usually this is done by measuring the IGF1 blood levels. These, however, cover a wide area. See graphic below:
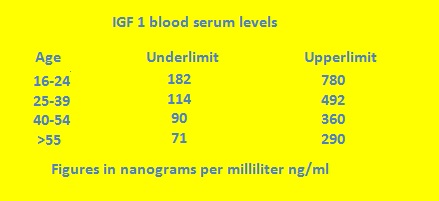 If one measures an IGF1 level of 290 ng/ml, then that is within normal limits for each age group. The huge spread is immediately obvious. The upper limit of >55 (290 ng/ml), still fits well within the range of the 16-24 age group.
If one measures an IGF1 level of 290 ng/ml, then that is within normal limits for each age group. The huge spread is immediately obvious. The upper limit of >55 (290 ng/ml), still fits well within the range of the 16-24 age group.
Take for example a person of 45 years with an IGF1 of 100, which fits just within the normal area. Then the doctor sees no problem and is not inclined to prescribe rhGH. Even if there are symptoms of GH deficiency in this patient, according to most protocols, he will not be treated. However, IGF-1 is not more than an indication. There are hundreds of patients described, that after a year or more on GH replacement have been refurbished: more energy, better skin, hair that grows back quickly, enhanced libido, improved cholesterol profile, increased bone density increased FFM [Fat Free Mass] decreased FM [Fat Mass] to name only a few notable physical effects of [long-term] GH administration. Yet by no means, in all these people a significant increased IGF1 serum level has been measured. Conclusion: the relationship between GH and GF1 is much more complicated than we initially assumed.
"No, not a panacea, but a wonderfully active hormone that after several weeks can turn zombie-like middle-aged people, into active and energetic people."
PEP
Here GH is used to improve performance. As a rule, this means to increase the muscle mass and strength. This is medically 'unethical', and why the hormone is listed on the doping list of the IOC and the appended federations. Exogenous administration of GH, however, can be detected. It is prohibited, just as well as the AAS, which is needed in addition to GH in order to attain a stable gain in strength and mass. It is known that off-season use brings a profit for the athlete during the competition season. And probably during many years (muscle memory), that’s why organizations are brainstorming how long to ban an athlete adequately after he has been caught using these hormones in the off-season (doping controls).
LEPLife Extension Purposes, also called Anti-Aging, called Age Management or Age  Control. The decrease of GH secretion by the pituitary gland almost linearly decreases with age. Unfortunately, this also applies to GH releasers. The sensitivity of the pituitary gland for glutamine and arginine is greatly reduced after the age of 40. If no releasers can be used, the only way to increase the GH serum-level is (to go around the hypothalamus and pituitary), by a direct administration of this hormone (injection). GH is prescribed as one of the hormones ( with testosterone, estrogen and melatonin and some others) as part of HRT (Hormone Replacement Therapy) by physicians. As a rule, they aim at long-term, or even better lifelong treatment. Dozens, if not hundreds of experiments have been described by researchers and the conclusion is almost always unanimous: beneficial effects on physical and psychological functioning and dose depending side effects, but mild ones such fluid retention, slightly increased blood sugar, joint pain (growth pain, I call that) and carpal tunnel syndrome, are the most commonly described ones. Insulin resistance slightly less. Almost always the sides reduce after a few months of use, especially with dose reduction.
Control. The decrease of GH secretion by the pituitary gland almost linearly decreases with age. Unfortunately, this also applies to GH releasers. The sensitivity of the pituitary gland for glutamine and arginine is greatly reduced after the age of 40. If no releasers can be used, the only way to increase the GH serum-level is (to go around the hypothalamus and pituitary), by a direct administration of this hormone (injection). GH is prescribed as one of the hormones ( with testosterone, estrogen and melatonin and some others) as part of HRT (Hormone Replacement Therapy) by physicians. As a rule, they aim at long-term, or even better lifelong treatment. Dozens, if not hundreds of experiments have been described by researchers and the conclusion is almost always unanimous: beneficial effects on physical and psychological functioning and dose depending side effects, but mild ones such fluid retention, slightly increased blood sugar, joint pain (growth pain, I call that) and carpal tunnel syndrome, are the most commonly described ones. Insulin resistance slightly less. Almost always the sides reduce after a few months of use, especially with dose reduction.
In the beginning, scientists worked with doses of about 5 IU p.d. in GH deficient adults. Cascade the dosage was reduced. Now one normally recommends an active dose of 0.3 to 0.9 IU per day, which may be administered almost without any side effects. Literature in reputable medical journals is sufficient. And everything points to favorable effects. From Rudman Effect of Human Growth Hormone in people over 60 years old New England Jounal of Medicine 1990. Just like Brazilian study (co-funded by Novo Nordisk (Norditropin®) where they worked with no more than 0.6 IU p.d. for 12 months.
Doses within the three domains: MEP
*GH deficiency in children: 0.5 ot 0.7 IU per kg body weight. This is equivalent to doses between 15 and 30 IU per week.
*Turner syndrome: 1.0 IU per body weight per week. That results in between 30-50 IU per week.
*Renal insufficiency: 1 IU per kg, also results to somewhere around 40, 50 Units.
*GH deficiency in adults: between 0.3 and 0.9 units per day. Up to 10 IU per week.
*After major surgery: 12 IU per day from the 2nd until approximately the tenth day after surgery.*With burns and some other disorders: applied locally: on the wound. Three times daily 0.2 - 0.4 IU per square centimeter (cm²).
PEPThe most difficult area, because we cannot rely on scientific research with athletes. Here the eternal ethics comes back into play. Simply no permission is given for experiments ( with often considerable doses) GH administered to healthy athletes. Not rest me other than to rely on practice: minimal effective dose of 1.5 IU per day, increasing to four, at most 6 IU. Higher doses do not appear to provide additional benefits, but provide more side effects.
LEP
At MEP I already mentioned a dose of GH deficient adults. I think that may be slightly higher (1-2 IU per day). Some anti-aging specialists recommend anyone over 40 years to begin with GH injections. Perhaps somewhat exaggerated. But if someone in his or her 40’s start using therapeutic use of rhGH, aging in the decades thereafter will be slowed. Before the age of 40-45 year, releasers still work well and it is therefore not necessary to use rhGH. Some Anti-Aging programs and rejuvenation therapy, recommend supplements in concert with other hormones like testosterone, estrogen, thyroxine (T4) Melatonin and DHEA improve performance and slow down the aging process. In addition, other OTC resources such as Ginkgo biloba, Glucosamine, Hydergine, Piracetam can be added.
Dose
Early adaptors of GH for bodybuilding and anti-aging suffered a number of side effects, including carpal tunnel syndrome, insulin resistance, type 2 diabetes, facial bone distortion, elongation of hands and feet, organ growth, etc. This was due to their inappropriate use of excessive doses, following the early treatment routines given to GH-deficient children (around 20 IU/day). This resulted in IGF-1 levels that were higher than the body could accommodate; most GH-related side effects can be managed by keeping IGF-1 values within or near the physiologic (normal) range.
 These early users also developed something we call a GH-GUT. HGH will bind to any receptors it can, including the organs and intestines, not just the muscles.
These early users also developed something we call a GH-GUT. HGH will bind to any receptors it can, including the organs and intestines, not just the muscles.
We hear of men and women using HGH at just 1-2iu’s a day and benefiting from it, and we hear of bodybuilders taking as much as 15+ iu’s a day and making DRASTIC changes in hyperplasia (development of new muscle tissue) and muscle growth. Nasser El-Sonbatty always said a pro-bodybuilder needed at least 15 iu HGH p/day. That’s why he used the nick GH15.
You need to ramp up dosages with HGH very slow, you don’t want to start off using 8 iu’s/day. The proper way to use HGH would be to start off with 2-3iu’s p/day for a solid month, then try to go to 4 iu’s p/day for another month, then ramp up to 6 iu’s p/day another month, etc etc.
Another issue nowadays is the legitimacy of HGH and knowing that what you have is real and dosed properly. This makes trying to even run it at a replacement dosage difficult.
The dosage depends on the goal. People generally use 2 IU per day for anti-aging purposes, between 4 to 6 IU for bodybuilding, weight loss and fitness, between 8 to 16 IU is used for short duration to treat severe burns or recover after injuries.
 Doses below 3IU per day usually bring no side effects while people can notice the improvement of their skin, better sleep, more energy, eating junk food without gaining weight, etc.
Doses below 3IU per day usually bring no side effects while people can notice the improvement of their skin, better sleep, more energy, eating junk food without gaining weight, etc.
After several weeks at 4IU and above some people will start to feel some side effects of somatropin (HGH). Slight water retention can be noticed in your fingers, toes and face (HGH makes the muscle cells hold more water and are thus temporarily inflated). Some people occasionally feel tingling sensation in their fingers and palms - this is known as carpal tunnel syndrome.
In practice carpal tunnel syndrome is the only side effect which actually bothers the user. Most athletes simply ignore it and continue the cycle for as long as they can. If the carpal becomes unbearable, they lower the dose or discontinue use until the side effects are gone. It usually takes about 2-3 weeks for the carpal tunnel syndrome to completely disappear.
When using 4IU and above, it is good to split the dose in two daily injections. Half in the morning and the other half in late afternoon. You should avoid taking HGH before bedtime because the body releases its endogenous HGH (3rd dose) when you falls asleep. If you take the dose before bedtime it might interfere with your endogenous HGH release.
Is GH the panacea of the future?
The enthusiasm of a number of doctors and researchers seem exaggerated. If one looks to the results to be achieved in the context of LEP than is the overwhelming number of beneficial effects and sometimes almost unlikely. For example, examination of the Flemish Endocrinologist Thierry Herthoghe calls after two months of treatment with an average of 0.75 IU also be thicker and fuller head of hair, increased skin elasticity, thickening of atrophied mandibles, reduce wrinkles on the face ... go yet but just by . Gene Science predicts that Jintropin® after 6 months will improve eyesight. Look, we have to be equally critical: perhaps can farsightedness, a consequence of aging, can be adjusted, albeit after much longer periods than half a year. Who in childhood had been sighted, do not have to rely on that GH defect or will raise equally. Grow faster and fuller head of hair: It's true ... but ... with it you cannot just connect to the conclusion that even in bare spots new hair will grow. That does not happen. Also warning words heard from the medical angle.
Summary
Proper synthetic HGH has been in recreational use for nearly 30 years and it never hurt anyone, except the big pharma who lost out on the profit due to the cheaper Asian competition undermining their overpriced grip on the western markets. Chinese manufactured HGH is identical or possibly even superior to the western big pharma produced HGH. If for no other reason than due to the simple fact that the competition among Chinese manufacturers is greater – they don’t hide behind copyrights, licenses and undermine each other by lawsuits and legal obstacles. They battle it out in the market
Because of the broad array of usage, the demand for GH will continue to grow strongly.
Translation of an older Dutch article.