
Dose and Duration

Its actually quite logic that if we use means that are bad for our organs, it makes a difference how long we do that and at which dose. A long heavy dosed cycle should do more harm than some short light cycles. We also know that injectable roids are safer than orals. And some orals, like Oxymetholone, are more hepatotoxic than others. The same is true for injectables, most of us know that the trenbolones do more harm than the testosterones. But how much harm will they do? I made a comparison for you with two case studies. One from a young bodybuilder on a low cycle and one from a professional bodybuilder with a long and heavy cycle.
Case presentation
T his case study presents a 23 year old male bodybuilder who, with a healthy history, incorporated the use of anabolic steroids into his training program for an upcoming competition. The subject administered both oral and parenteral forms of steroid over a 6 week period. Serum and urinalysis were conducted before, during and after a six week interval of steroid administration. In addition, the subject recorded his subjective side effects during this period.
his case study presents a 23 year old male bodybuilder who, with a healthy history, incorporated the use of anabolic steroids into his training program for an upcoming competition. The subject administered both oral and parenteral forms of steroid over a 6 week period. Serum and urinalysis were conducted before, during and after a six week interval of steroid administration. In addition, the subject recorded his subjective side effects during this period.
At 7 weeks pre-competition, the athlete initiated an anabolic steroid program for a 6 week period. He discontinued his drug use 1 week prior to competition.
During the initial 3 week period, the subject administered parenteral agents, Nandrolone Deconoate 300 mg/wk, Bolasterone 30 mg/wk, and Mesterolone, which is an oral compound but is altered at the 17-beta position so that it possesses pharmacological characteristics similar to an injectable steroid (25 mg/day).
During the next 3 weeks of therapy, the steroid types used were ones which were associated with less water retention and therefore, minimized the "bloated" appearance which is an undesirable state for competition. These included most of the oral preparations which have short side chains at the 17 alpha position of the steroid molecule. The drugs in this phase included Mesterolone 50 mg/day, Oxandrolone 35 mg/day, Boldenolone Undecylenate 150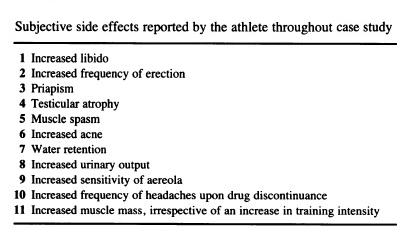 mg/wk, and Methenolone Actate 60 mg/wk.
mg/wk, and Methenolone Actate 60 mg/wk.
Serological assessments were completed prior to initiation of anabolic therapy, twice during the 6 week drug session and at five and 13 weeks following discontinuance of drug use. The results of these tests are recorded in the table below. Also recorded were any subjective side effects noted by the athlete.
Discussion
U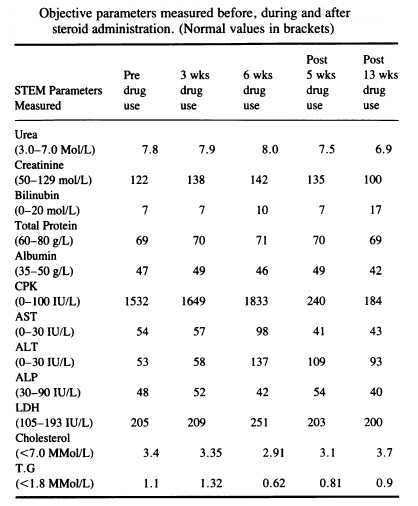 rea values were elevated throughout the entire study period. This was likely due to the high protein intake of the athlete and not necessarily attributed to any degree of renal dysfunction.34 Creatinine, also a kidney function test, was elevated throughout most of the study with the exception of 13 weeks post drug use.
rea values were elevated throughout the entire study period. This was likely due to the high protein intake of the athlete and not necessarily attributed to any degree of renal dysfunction.34 Creatinine, also a kidney function test, was elevated throughout most of the study with the exception of 13 weeks post drug use.
Creatinine excretion was consistent in a given time period and was proportional to the increased amount of muscle mass acquired by the subject. Table 2 reveals a steady increase in creatinine excretion from the non-drug use state to the high point of drug consumption and then steadily diminished thereafter. This seemed logical since the athlete acquired muscle mass in proportion to the creatinine increase. The subject trained little from the day of competition to the 13 week post period and hence lost approximately 10 pounds of muscle mass which was reflected by diminishing creatinine levels.
Bilirubin remained normal throughout the study suggesting undisturbed liver bilirubin metabolism. Total protein and albumin changes, in this study, were also unremarkable.
Creatinine phosphakinase (CPK) determinations were highly elevated throughout the drug use period but decreased markedly in both the non-training and non-drug use periods. The elevated titres of CPK were attributed to muscle damage induced by severe exercise 35'34 (4-5 hours daily) and to the intramuscular injections administered by the subject. During the pre-steroid phase, CPK titres were lower than both the 3 week and 5 week drug stages. An elevation of 301 IU/L of CPK from the pre-steroid to the 5 week steroid stage was likely the result of the intramuscular injections since the intensity of training did not appreciably alter during these stages of the study.
The non-specific liver function tests (LFT's), AST and ALT, maintained higher than normal values throughout the entire study. Note, these values were elevated prior to anabolic therapy initiation. This was not surprising since both AST and ALT are found in skeletal muscle and are released into the serum when muscle damage is increased. This is explained in a manner similar to that of CPK elevation. Strauss et al studied 32 weightlifters of which 20 were using oral anabolics while the remaining 12 were not. The steroid subjects demonstrated ALT levels greater than normal and AST values on the high side of normal. The 12 individuals not using steroids, demonstrated ALT and AST levels virtually identical to those using the steroids.
Another study conducted by Hogermant et all of 5 weightlifters, 3 of which were taking steroids and 2 who were not, determined that all five lifters displayed elevated AST and LDH levels while ALT and ALP were normal. The studies suggest that intense weight training alone, can elevate non-specific LFT's.
At the peak of drug use, AST and ALT levels reached 98 and 137 IU/L, respectively. This could arise secondarily to the increased drug consumption at this stage of the study and/or to the change to the oral forms of steroids, namely Oxandrolone ( see below).
This specific drug, of course, has been associated with higher incidences of hepatotoxicity than the parenteral forms. Another hypothesis suggests that the elevation of LFT's is due to skeletal muscle breakdown rather than any hepatic dysfunction.
There are two aspects which reinforce this conjecture. One proposes that these elevations parallel those of CPK which reflects muscle damage due to exercise and intramuscular injections. Secondly, the specific LFT, especially alkaline phosphatase, remained within normal parameters throughout αthe entire study, even on the lower side of normal. It appears likely that a combination of all the above exists and that the latter factor, muscle breakdown, plays the largest role in the elevation of non-specific LFT's.
Total LDH levels were monitored and since this enzyme is found in skeletal muscle as well, it is not surprising that these changes parallel those of CPK. Haupt and Rovere suggest that measurement of the hepatic fractionation of LDH is a useful specific LFT. Biochemical analysis during this study did not include LDH fractionation, as such LDH was considered as a non-specific liver function test.
Both cholesterol and triglycerides (TG) levels were unremarkable throughout the study.
Urinalysis was similarly unremarkable.
Conclusion
In view of the measured results in this isolated case study, it was considered that the only noteworthy alterations in blood chemistry were CPK, AST, ALT, and LDH. It was also felt that
no pathophysiological processes were occurring with respect to liver dysfunction and that elevated non-specific LFT's were more a product of muscle breakdown induced by severe exercise and by intramuscular injection.
Case presentation II
I n 2012 a 37-year-old male professional bodybuilder with a body height of 180 cm and a body weight of 118 kg presented himself with increasing epigastric and abdominal pain to an outside department of hepatology.
n 2012 a 37-year-old male professional bodybuilder with a body height of 180 cm and a body weight of 118 kg presented himself with increasing epigastric and abdominal pain to an outside department of hepatology.
That are impressive figures other professional bodybuilders with an height of 5′ 11″ (180 cm) and an off season weight of 260 lb (118 kg) are Lee Haney and Miloš Šarčev.
For a period of at least five years he has been consuming the following AASs in a daily medication schedule:
Testosterone propionate, testosterone phenylpropionate, testosterone isocaproate, testosterone decanoate 250mg (Sustanon)
Trenbolone acetate 75mg
5alpha-androstanediol 100 mg (dihydrotestosterone (DHT) prohormone)
B oldenone and Methandriol dipropionate 240 mg (Drive or Overdrive)
oldenone and Methandriol dipropionate 240 mg (Drive or Overdrive)
Stanozolol 100 mg,
Oxandrolone 4×10 mg,
Letrozole 0,065 mg,
Oxymetholone 3 × 50 mg or Methandienone 10 mg.
Oxymetholone or Methandienone was discontinued three weeks before competition. In addition, he took Spironolactone 100 mg, Mesterolone 25 mg, Fluoxymesterone 10 mg four weeks, and Torasemide eighteen hours before competition. Furthermore, a daily intake of amino acid, vitamins, and mineral tablets, T4 (200 μg), and growth hormones (8 I.E.) was reported.
The nutritional protocol consisted of six small, protein-rich meals (chicken breast, fish, protein shakes, salad, vegetable, etc.), a high caloric and high protein-containing diet to build up muscle mass. Eight weeks before competition, the meals and consequently the caloric intake were reduced by 50% to reduce subcutaneous fat.
Torasemide, a diuretic, was taken to achieve a more muscular bodily contour by reducing extracellular and subcutaneous tissue volume.
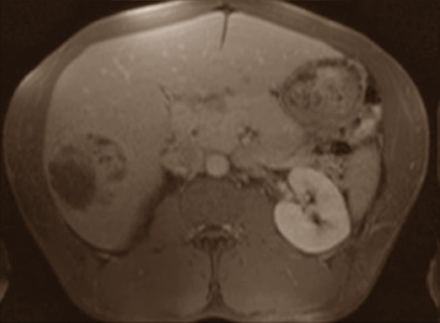
The physical examination of the professional bodybuilder revealed an athletic appearance with enhanced muscular contour. A mild tenderness in the right upper abdominal quadrant was found. Any history of alcohol consumption or smoking was denied. A hepatic lesion was discovered by abdominal ultrasound. It appeared as a predominantly hyperechoic lesion in the right lobe of the liver. The magnetic resonance imaging showed a hepatomegaly and confirmed the lesion which showed features of a hepatocellular adenoma[The dark patch below left.]. The patient was transferred to the Department of Visceral Surgery, University of Cologne for a laparoscopic resection of the suspected HCA.
 If steroids users develop liver tumours then they usually have hepatocellular adenoma: benign swellings that do not spread through the rest of the body. Nevertheless many doctors think it's a good idea to remove the swellings because they may start to bleed or could change into a more malignant form of tumour: hepatocellular carcinoma.
If steroids users develop liver tumours then they usually have hepatocellular adenoma: benign swellings that do not spread through the rest of the body. Nevertheless many doctors think it's a good idea to remove the swellings because they may start to bleed or could change into a more malignant form of tumour: hepatocellular carcinoma.
Hepatocellular carcinoma is liver cancer. This form of cancer is most common among alcoholics, but very rare among steroids users. That's why doctors at University Hospital of Cologne were surprised when they found hepatocellular carcinoma in this bodybuilder.
The doctors in Cologne decided to operate on the man. They removed the part of the liver where the tumour was located; the tumour itself measured 6 x 5 x 5 cm. In the lab they discovered that it was hepatocellular carcinoma that the man had developed.
In the literature the doctors only found 7 cases of bodybuilders who had developed hepatocellular carcinoma as a result of steroids use. The chance of steroids users developing this form of cancer is therefore small, but not zero.
"Bodybuilders who abuse anabolic androgen steroids over a long period of time have a risk of developing an hepatocellular adenoma or hepatocellular carcinoma and should therefore be well monitored", the doctors write. "Periodic hepatic ultrasound seems to be an adequate screening procedure to detect the development of hepatic lesions."
"Although most of the tumors developing by anabolic androgenic steroids misuse or intake are benign, early detection is important in order to avoid the associated risk of malignant transformation and life-threatening hemorrhages", they continue. "In these cases a surgical excision is recommended."
Fortunately the bodybuilder in the study recovered. Just seven days after his operation the doctors sent him home and when they examined him 27 months later he was completely healthy.
Oxandrolone
A growing number of reports about abuse of anabolic androgen steroids in Western Europe and the USA by competitive and noncompetitive bodybuilders is reported in the literature. A correlation between AAS use and hepatocellular adenoma has been increasingly recognized in athletes taking AAS. While danazol is associated with hepatocellular adenoma formation, other preparations like oxymetholone, respectively, methyltestosterone can lead to hepatocellular carcinoma. In addition to other synthetical androgenic steroids, the 37 year old bodybuilder in the case study above consumed the prospective carcinogenic oxymetholone (50mg) three times a day.
 There is one reported case of a steroid induced hepatic tumor in an athlete resulted in his death. This was a male bodybuilder who succumbed to hepatocellular carcinoma and hepatic cholangiocarcinoma.
There is one reported case of a steroid induced hepatic tumor in an athlete resulted in his death. This was a male bodybuilder who succumbed to hepatocellular carcinoma and hepatic cholangiocarcinoma.
The athlete employed both oral and parenteral compounds for four years preceding his death including; Methandrostenolone (oral), Oxandrolone (oral), Stanozol (oral), Methenolone and Nandrolone Decanoate (administered intramuscularly).
This individual utilized the 17-alpha alkyl derivatives of testosterone for a protracted period of time, as was the case with almost all of the other reported instances of hepatic tumors attributed to the use of anabolic steroids. It is significant to note that Oxymetholone (Anadrol) was the preparation most frequently associated with the incidences of both peliosis hepatis and hepatic carcinoma.
It will be clear by now but, … extended use of high doses of oral anabolic steroids can cause liver tumors or hepatocellular adenoma. We might call this 'liver cancer', but doctors would not use this term here. Real liver cancer, in which liver cells mutate into cancer cells, is even more rare among steroids users than hepatocellular adenoma. But it does happen, report doctors at the University Hospital of Cologne.
Cholestasis, peliosis hepatis and liver tumours, are the possible consequences of steroid use for the liver. Cholestasis is a condition whereby the liver can no longer remove waste products via the bile to the intestines. Faeces become grey, skin colour yellow, you start to itch and if you don't receive treatment quickly your liver tissue starts to die off.
Peliosis hepatis is a condition in which blood filled cavities form in the liver. It was probably the cause of death of Andreas Muenzer. Doctors don't yet know how peliosis hepatis arises, but they do know how to treat the problem: you just need to remove the cause. If Andreas Muenzer had stopped taking steroids in time he could very well still be alive today – and his liver would have recovered.
What we can do is ..if you want to use oral steroids as a kickstarter for your cycle or in the cut, don’t combine it with recreational drugs, oral medication, alcohol. And use your liverprotectors LIV 52 or/and Milk Thistle (Silybum marianum), and not because I say so. Educate yourself !! Read all you can about the subject and discuss it on our forums.
