
Bulking and pre-contest drugs and diet of South African bodybuilders during contest season 2010.

 We read a lot on the discussion boards and magazines about the use of drugs, the trainings and diet protocols of the bodybuilders. The bodybuilders in this research are no professionals. They are competing in the senior men’s division of International Federation of Body Building South Africa (IFBBSA). All the athletes registered with the (IFBBSA) were invited to participate in the study. More than 200 invitations were sent out to the existing database – only 19 athletes conveyed their interest in participation. Eventually, only 14 athletes partook in the full protocol. They competed on Provincial and National contests in different weight categories. What makes it really interesting is the fact that the researchers captured all information in schemes. Of course most readers are particular interested in the drug protocols, we call cycles. You’ll find some at the end of this blog-post. It also shows the huge difference in doses. The study also shows the influence of diet –heavy training and diet on blood-pressure, kidneys, liver and other organs.
We read a lot on the discussion boards and magazines about the use of drugs, the trainings and diet protocols of the bodybuilders. The bodybuilders in this research are no professionals. They are competing in the senior men’s division of International Federation of Body Building South Africa (IFBBSA). All the athletes registered with the (IFBBSA) were invited to participate in the study. More than 200 invitations were sent out to the existing database – only 19 athletes conveyed their interest in participation. Eventually, only 14 athletes partook in the full protocol. They competed on Provincial and National contests in different weight categories. What makes it really interesting is the fact that the researchers captured all information in schemes. Of course most readers are particular interested in the drug protocols, we call cycles. You’ll find some at the end of this blog-post. It also shows the huge difference in doses. The study also shows the influence of diet –heavy training and diet on blood-pressure, kidneys, liver and other organs.
In short the effects and side/effects of AAS and ancillaries on the body composition, blood values and the organs of the athletes
 Blood assays were performed on each athlete on 3 different occasions, while anthropometric measurements and blood pressure readings were taken on 4 different occasions over the length of the competitive season. Each individual athlete recorded his AAS abuse, while some athletes provided sample diets as well.The bodybuilders where followed under full pre-contest preparation conditions. It should also be understood that body builders under full pre-contest preparation will respond differently to the use of special diets, different training strategies and different types of AAS abused, than compared to when they train under normal out-of season conditions.
Blood assays were performed on each athlete on 3 different occasions, while anthropometric measurements and blood pressure readings were taken on 4 different occasions over the length of the competitive season. Each individual athlete recorded his AAS abuse, while some athletes provided sample diets as well.The bodybuilders where followed under full pre-contest preparation conditions. It should also be understood that body builders under full pre-contest preparation will respond differently to the use of special diets, different training strategies and different types of AAS abused, than compared to when they train under normal out-of season conditions.
Anecdotally, when preparing for a competition, most elite body builders in South Africa will go through two totally different phases of training and dieting. The first phase is the bulking- or weight-gaining phase. During this phase, a structured diet with high carbohydrate component and moderate to high fat content will be followed for several months. The diet will be followed fairly strictly, but food portions will mostly not be weighed. Training schedules are fairly strict, with heavy weight training and very little aerobic work done. Body skin fold fat % is generally kept between 12-14 %, but some individuals may let that increase to 15-18 %.
The weight-gaining phase
During the weight-gaining phase, AAS substances are used in moderately high doses compared to the pre-contest period. Substances of choice are the testosterone esters, especially the longer acting enanthates and cypionates, as well as the testosterone derivatives like boldenone (Equipoise) in its longer ester forms. The oral testosterone derivatives are either 17-alkylated or 17-methylated in order to pass the first liver metabolism. Substances include methandrostenolone (Dianabol), fluoxymesterone (Halotestin), 4-chlorodehdromethyltestosterone (Turinabol). The 19-nortestosterone derivatives, namely nandrolone (Deca-Durabolin) and all its shorter and longer esters are used commonly during this phase. These substances are used in different combinations simultaneously, over periods of 6 weeks to as long as 24 weeks. These periods are commonly referred to as “steroid cycles”.
The pre-contest phase
The second phase of training and dieting, is called the pre-contest preparation phase. This is a very intense phase of high volume training, consisting of numerous protocols of isolation-type exercises, combined with daily aerobic workouts. This phase usually starts about 16-13 weeks from the time of the competition. The length of this phase will be depending on the athlete’s experience at pre-contest prep, his body fat % being less than 12-14 % and his weight category to be competed in. Generally the larger athletes will start their pre-contest preparation at 20 weeks before competition. During this phase, extremely strict, structured diets are followed, with each meal being weighed. Calorie intakes are calculated according to formulas and the ratios of protein, carbohydrates and fats are changed intermittently. Weekly body fat % assessments are done, followed by calorie adjustments for the following week. High protein-, very low carbohydrate and moderate fat diets are mostly used, but this is highly individualised.
During the pre-contest phase, a multitude of chemical substances are abused to enhance the desired physique – this strategy of using combinations of different classes of drugs, is called “stacking”. This will be the period with the highest AAS substance milligram usage per week, in order to have the highest anabolic effect of nitrogen retention to protect the lean body mass gained during the bulking phase, while different ergogenic substances are used for the catabolic process of fat burning. The AAS substances of choice during this phase are usually injectable substances with very short acting esters like the propionates and acetates. Most, if not all of the “cycles” used, will include some form of injectable testosterone, usually combined with the 19-Nortestosterone derivatives Trenbolone, which seems to be a favorite pre-contest body building drug amongst this group of athletes. Athletes will tend to use AAS substances that generally do not aromatize, as this will lead to unwanted estrogen production and subsequent water retention and subcutaneous fat deposit. For this reason, most athletes use the class of substances derived from dehydro-testosterone. These are oxandrolone (Anavar), drostanolone (Masteron), methenolone (Primobolan), mesterolone (Proviron) and stanozolol (Winstrol).
The difference between medically used and recreational abuse, lies in the dosage and interval of administration of these drugs. Medically used AAS is aimed at replacement therapeutic dosages (in hypogonadal men 6-10 mg/d is used), prescribed on a continuous basis, or with regulated intervals of usage. However, the AAS abusers use very complicated drug protocols of different AAS drugs simultaneously, which is increased at dosages as high as 40-100 times more than levels needed to reach physiological homeostasis. The perceived belief for the physiological basis for using the stacking method is to maximise the androgen receptor binding by using different drugs having different binding affinities to the androgen receptor. By 2005, no scientific research clearly showed such an effect through the use of stacking protocols. Stacking would usually continue for periods of 4 to 18 weeks on average, although it has been noted that athletes use stacking protocols continuously for as long as 30 weeks over a competitive season. After the cessation of such a stacking cycle, athletes would generally take a drug holiday of anything from 1 to 12 months
AAS Cycle Length and Dosages
The Androgen status of the cohort was not controlled, as ethical considerations precluded the investigator’s involvement in drug administration. For this reason, the information on AAS abuse and cycles were anecdotally obtained from the present cohort’s athletes who were already abusing self-sourced AAS.
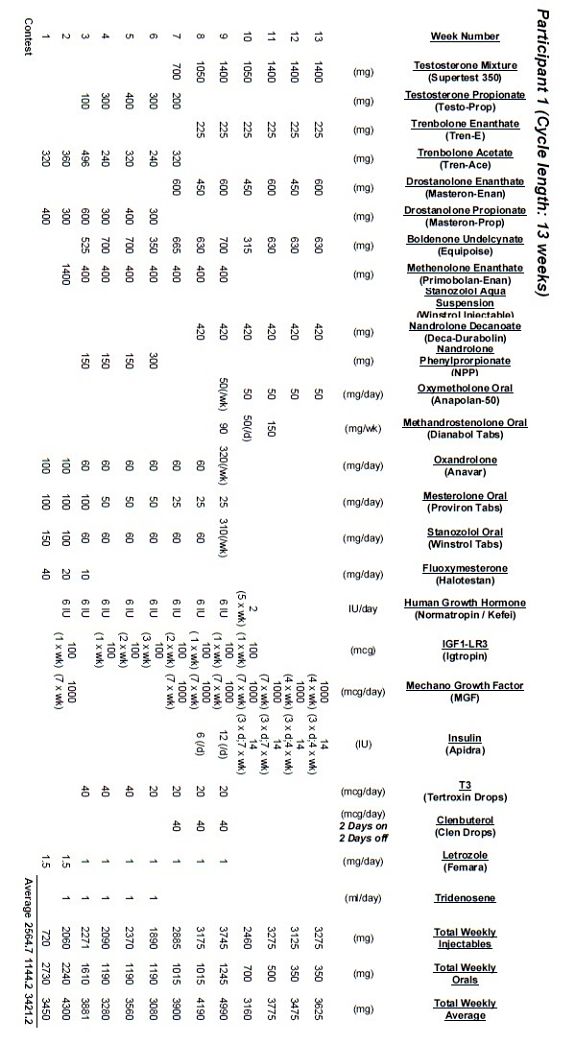
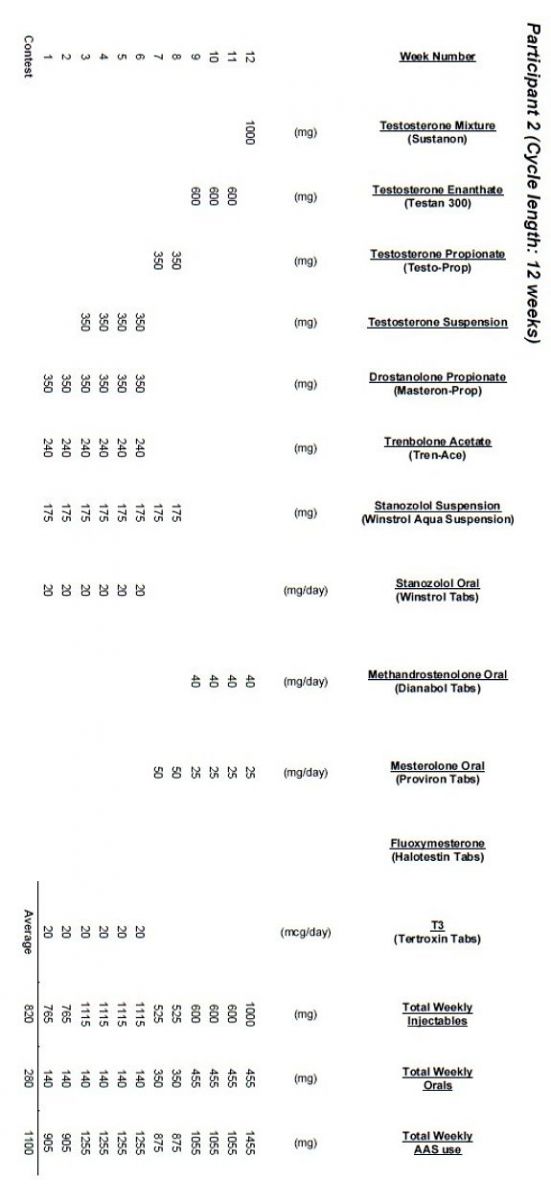
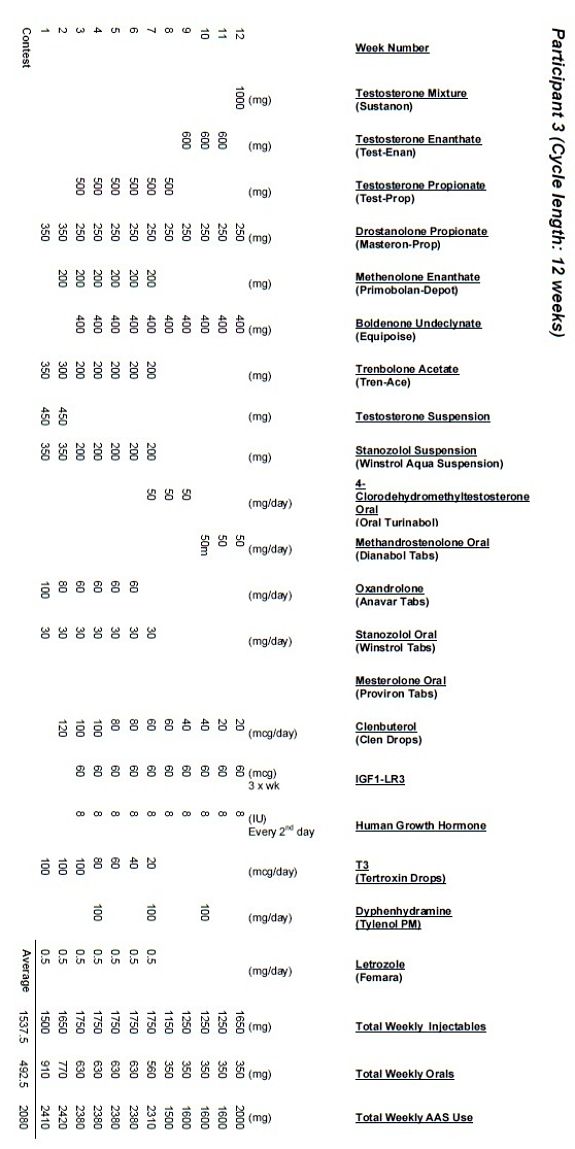
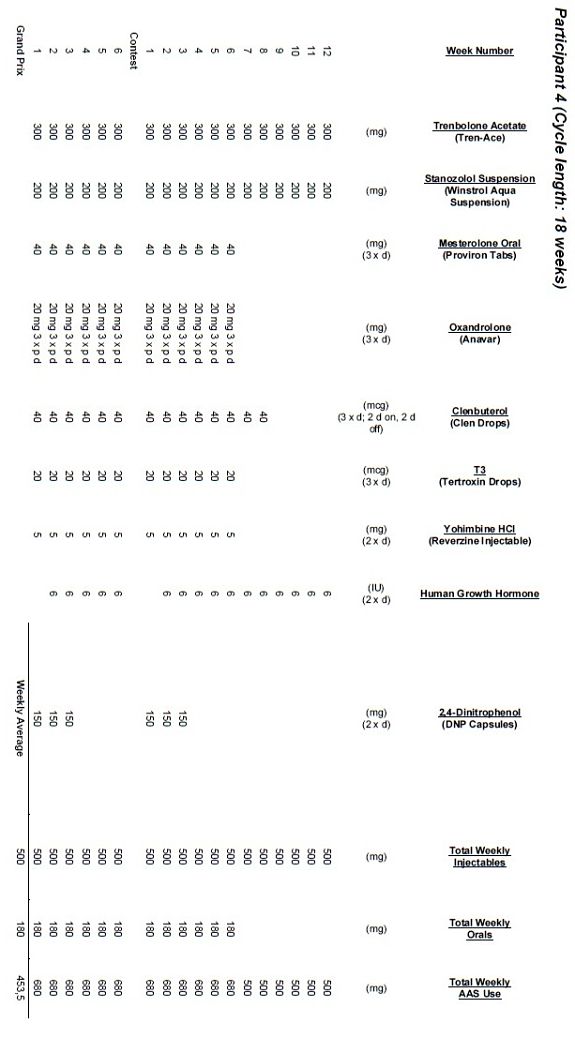
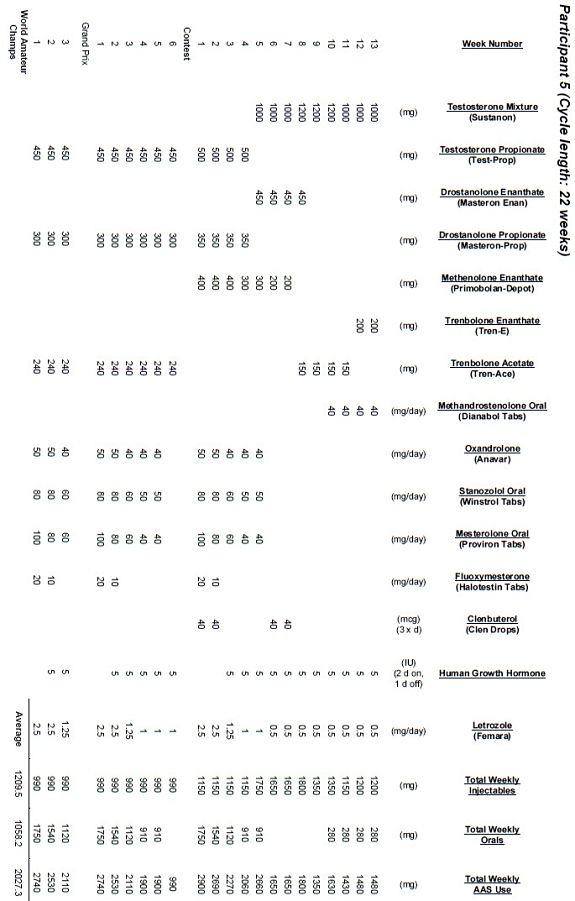
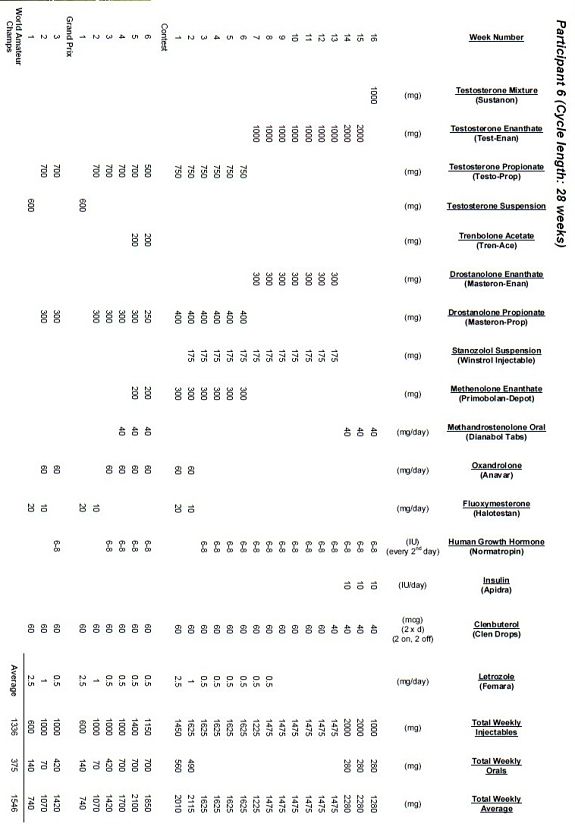
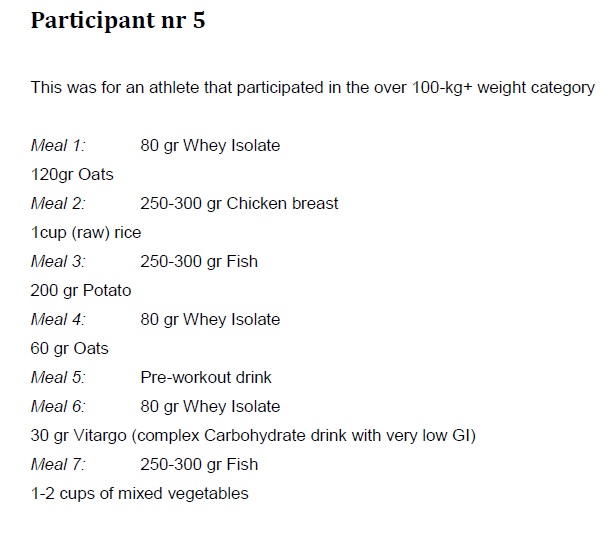
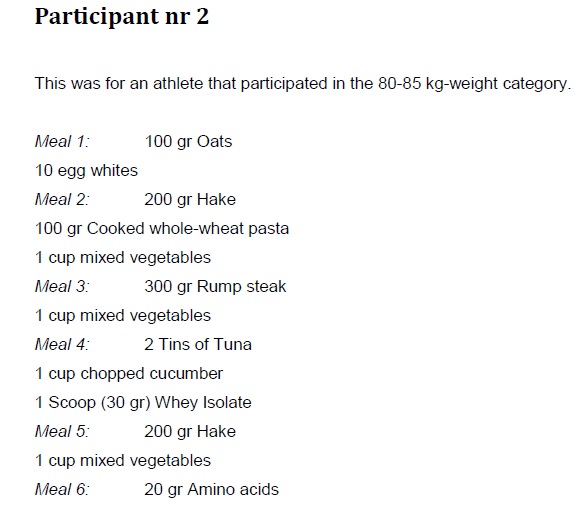
Dosages of the different AAS drugs abused, as well as the cycle lengths, were recorded for each participant in the cohort (Annexure B). Most of the participants abused AAS drugs sourced from illicit underground steroid sources, some participants sourced some of their AAS drugs from legal pharmacies, while one particular participant only used pharmaceutical grade AAS drugs sourced from legal pharmacies. This participant used drugs averaging doses similar to that of the rest of the cohort. The body composition and blood profile changes in this athlete’s case were not much different to that of the rest of the cohort’s participants.
The mean AAS cycle length for the cohort was 17.43 weeks, with the shortest cycle of 12 weeks and the longest 25 weeks. The mean weekly injectable AAS abuse for the cohort measured 1179.81 mg, with the lowest average 333.3 mg per week and the highest 2564.7 mg per week. The mean weekly oral AAS consumption for the cohort measured 573.47 mg, with the lowest average 180 mg per week and the highest average 1144.7 mg per week. The mean total AAS abuse per week for the cohort measured 1638.3 mg, with the lowest average 453.5 mg per week and the highest average 3421.2 mg per week. Though it might have been expected that the heavier athletes would use higher doses, it was not the case in the present study. Some of the higher weekly doses were consumed by athletes competing between the 80kg to 100kg weight categories. One particular athlete in the 90kg to 100kg category, consumed on average close to twice the doses of AAS used by the athletes competing in the over 100kg category.
.jpg)
On this scheme two values are compared. It’s obvious that the total doses of anabolic steroids don’t always correlate with the body weight of the bodybuilder. Thus that the heaviest bodybuilders use the highest doses of anabolic steroids. It’s a pity that we don’t have pictures from the athletes nor know on which level they compete. It’s a very long study and I’ll use more info in later blogposts.
Liver values
It is thus clear from the present study’s findings that some of the observations correlate well with observations from other studies in the literature, but that some of the findings differ from what has been documented before in the literature. However, it should be noted that the present study’s cohort differed vastly from cohorts from other studies in the literature, as none of the latter observed cohorts under full pre-contest preparation conditions. In conclusion, it should be understood that body builders under full pre-contest preparation will respond differently to the use of special diets, different training strategies and different types of AAS abused, than compared to when they train under normal out-of season conditions.
Muscularity may cause increases in the transaminases. In such cases, this will usually be shown as an AST/ALT-ratio of > 1.0. However, in the AAS abusers, it is commonly noted that the ALT values are on average higher than the AST values – primarily as a manifestation of AAS-induced liver function impairment.
The most commonly used measures of hepatotoxicity include AST, ALT and Lactate Dehydrogenase (LDH). These values are usually in the range of two and up to three-fold the normal values. These levels are very similar as to those seen as side effects to combined oral contraceptive usage in women. The most sensitive marker to hepatobiliary disease and obstruction is the GGT level.
The peak in AST, ALT and GGT levels usually would occur after 2-3 weeks of AAS consumption. These levels would return to baseline levels after a few weeks up to three months after AAS abstinence. In the review article by Kutscher et al in 2002, it is stated that the reversible course of liver enzyme elevations explains the reason why athletes opt to abuse these drugs in a cyclic manner. However, when the AAS is administered for at least one month continuously, but generally greater than 2 to 5 months, dose-dependent jaundice and hepatic dysfunction are more likely to develop. The cyclic administration of AAS can thus reduce the subsequent liver toxicity.
Levels of serum liver enzymes are more the indicators of the hepatocyte integrity or cholestasis, rather than liver function itself (Scally, 2008). A decrease in liver functioning mass can be more accurately assessed by changes in clotting times or serum protein levels. There is no single, simple test that can assess overall liver pathology. AST and ALT are the most sensitive indicators of hepatocellular injury, indicating hepatocellular necrosis or inflammation. ALT raises the most dramatically in acute liver disease. The magnitude of the elevation has no prognostic value; neither does it correlate with the degree of liver damage. AST is relatively nonspecific and rises acutely in myocardial infarction, heart failure and muscle injury, but high levels indicate liver cell injury. Most liver diseases will show AST increases that are less than that of the ALT increases (AST / ALT-ratio 1.0). In AAS abusers, the AST and ALT level increases correlate significantly with the extent (duration and weekly dosage) of AAS abuse.
Conclusion
The present study showed that, despite high doses of AAS that were abused, blood pressure could be fairly well controlled, due to the high volumes of aerobic training that were combined with the normal resistance training protocols generally followed by body builders. The results from this study also suggests that the pre-contest body builder loses fat stores, as well as lean mass simultaneously, when preparing for a competition – this despite very high doses of AAS abused. It should be noted that the literature generally associates AAS use or abuse with the acquisition of lean mass. However, these studies used standardised energy intakes, exercise doses and testosterone administration, with participants mostly not under the same strenuous physiological strain under which the competitive body builder prepares for a competition. In the present study’s cohort, the AAS doses were not standardised, as the drugs were mostly sourced from illicit origin – this may have contributed to results differing from that found in the studies using standardised protocols.
Due to the ethical considerations, the different AAS drugs used by the participants could not be provided in standardised doses to them. Thus, content of the oral and injectables used in the present study, was unknown. It may be feasible in future studies to ask participants to willingly provide some of these preparations for analytical biochemistry in an accredited laboratory – a grant to finance such an endeavour could be applied for.
A number of risk factors for disturbed carbohydrate metabolism were noted – 71,4 % of the participants had BMI 25, combined with HDL levels 0.9 mmol/l. The degree to which AAS abuse contributed to the development of pre-diabetic status in some participants is unclear and needs future investigation. The unchanged or even decreased cholesterol levels observed in the present study were due to participants performing a greater deal of aerobic exercises, probably counter-balancing the cholesterol increasing side effects of the AAS abuse. However, the AAS induced decrease in HDL levels was not counter-balanced by the high aerobic exercise doses. The extent to which disturbed liver function, the AAS choices abused and concomitant abuse of estrogen blocking agents contribute towards these findings, are unclear and needs further investigation. The finding that the Total Cholesterol/HDL-ratio decreases over the length of the study, implying a decrease in cardiovascular risk despite the abuse of high doses AAS for extended periods of time, may render a false sense of security to the general body builder abusing AAS. It should be noted this decrease was probably multi-factorial and that the full extent of high dose AAS abuse continuously or intermittently for extended periods of time over many years, have not been fully investigated as yet. If the opportunity arises, future longitudinal studies should especially investigate the clinical significance of repeatedly impaired blood lipid profiles in AAS abusers.
The researcher concluded that the main cause for the liver enzyme changes in the cohort, seem to have been AAS-driven, evidenced by the increase seen in GGT and the disproportionate increase in ALT values compared to AST values increase. At the one-week post-competition measurement, 4 participants presented with AST levels lower than at the onset of the pre-contest period – the researcher could not find any explanation for this. Physicians engaged in the long-term follow-up of body builders, should steadfastly adhere to the WHO guidelines for the treatment of drug-induced liver disease. It would be unwise to consider any enzyme increases in the absence of a diagnosis as being non-significant. The researcher suggests regular follow-up of liver enzymes in all AAS abusers.
In the present study, a uniform group of participants were identified, whom all used short-acting AAS esters around the time of competition – they all had hypogonadotrophic hypogonadism (the combination of lowered FSH, LH and testosterone levels), which contributed towards them gradually losing lean mass in the weeks after the competition. The Androgen Status of the cohort was difficult to control, as ethical considerations precluded the investigator’s involvement in drug administration. For this reason, only anecdotal information was recorded. The mean injectable AAS weekly abuse was recorded to be 1179.81 mg; the mean oral AAS weekly abuse was 573.47 mg, while the mean total AAS abuse per week measured 1638.3 mg.
It should be noted that the present study’s cohort differed vastly from cohorts from other studies in the literature, as none of the latter observed cohorts under full pre-contest preparation conditions. It should also furthermore be understood that body builders under full pre-contest preparation will respond differently to the use of special diets, different training strategies and different types of AAS abused, than compared to when they train under normal out-of season conditions.
Due to the lack of any longitudinal studies on the adverse effects of long-term AAS abuse, the long-term implications of AAS abuse on health is still unknown. Mostly, the emphasis of the sports medicine literature is on the methods of detection of the newest medications that athletes are currently using. The South African Medical Community has very little knowledge on the types of AAS substances and the dosing protocols abused in general amongst the elite, competitive Body Building athletes in South Africa.
The potential physiological, psychological and health implications due to the AAS abuse amongst body builders are factors that warrant continuous future attention by investigators, as well as sports physicians. The sports physicians should continuously target their efforts at counselling adolescents and other athletes about the potential long-term harms of AAS abuse, as well as regularly and prudently follow-up on the potential adverse effects that may develop in current AAS abusers.
To summarize:
Along with the concomitant abuse of high doses of AAS over extended periods, the present study also found:
*Minimal changes in blood pressure
*Initial decrease in lean mass, followed by rapid increase in lean mass in just one week and failure to maintain that gain over the following weeks
*Disturbed carbohydrate metabolism with increased risk for pre-diabetic status
*Lipid profile changes, with decreased HDL, unchanged Total Cholesterol and decreased LDL
*Liver enzyme changes highly suggestive of AAS-driven adverse effects
*Hypogonadotrophic hypogonadism status
*Very high Androgen Status for the cohort with mean total AAS abuse per week measuring 1638,3 mg, with average AAS cycle lengths of 17.43 weeks.
Source: Body Composition and Blood Measurements of Elite Senior South African Body Builders during the Competitive Season 2010 by Dr. R. Barnard.
- Login to post comments