
ART ORAL CRYSTALLINE

ART ORAL CRYSTALLINE
A new way of using an old Hormone
 Just like with us some scientists are really interested in effect of anabolic steroids with or without recombinant Growth Hormone, maybe not for the same reasons it interests us, but their research is very interesting for us iron adepts. The research results from Professor Ken Ho and Dr. Vita Birzniece are discussed in many discussion-forums, but not that many people on the forums are aware of the full impact of the results. Just look at the broad line of their research on the somatropin axis – doping – testosterone and application and doses.
Just like with us some scientists are really interested in effect of anabolic steroids with or without recombinant Growth Hormone, maybe not for the same reasons it interests us, but their research is very interesting for us iron adepts. The research results from Professor Ken Ho and Dr. Vita Birzniece are discussed in many discussion-forums, but not that many people on the forums are aware of the full impact of the results. Just look at the broad line of their research on the somatropin axis – doping – testosterone and application and doses.
What is actually very interesting in their research, is the fact that the active pharmaceutical substance is pure crystalline testosterone. Is this completely new? No, of course not because the raw powders is where it all started after isolating testosterone from testicles and later when scientists were able to synthesize testosterone. Research on unmodified testosterone is scares, because most research is funded by the pharmaceutical industry and they can’t patent bioidentical testosterone, thus have no reason to fund research. Still you can find studies, like Bioavailability of oral testosterone in males Frey et al 1979:
“Twenty-six male volunteers received a single oral dose of testosterone as free crystals or as the undecanoate ester. A significant and reproducible rise in serum testosterone level was found after ingestion of free testosterone.”
In older blogposts I showed how, on labscale, you can purify and crystalize raw powders of testosterone base. Also in an older blogpost I explained how you can complex these purified and crystalized powder with hydroxypropyl-beta cyclodextrin (HPBCD), to improve bioavailability. Both links are beneath this blogpost.
Is this only possible with testosterone basic powder. Nope, I also posted some old research on methandrostenolone (methandienone - Dianabol) on crystalizing (acetone) and dosing and compounding. But back oral testosterone.
A smart way of using testosterone to prevent muscle wasting
 Research from Professor Ken Ho , Dr. Vita Birzniece et al, suggests that a small dose of testosterone directed solely to the liver stimulates protein synthesis, likely preventing muscle loss and wasting, and potentially promoting muscle growth. The researchers believe they have developed a safe and effective treatment for men and women, that could prevent the muscle wasting associated with many chronic diseases and with ageing (Anti-aging -hypogonadism)
Research from Professor Ken Ho , Dr. Vita Birzniece et al, suggests that a small dose of testosterone directed solely to the liver stimulates protein synthesis, likely preventing muscle loss and wasting, and potentially promoting muscle growth. The researchers believe they have developed a safe and effective treatment for men and women, that could prevent the muscle wasting associated with many chronic diseases and with ageing (Anti-aging -hypogonadism)
 The Australian team showed in healthy postmenopausal women that a small dose of the male hormone testosterone prevented protein wasting. The pure crystalline testosterone, taken orally, went straight to the liver, and the dose (40mg/day) was small enough to ensure it was contained there, with no spillover to the bloodstream and other organs.
The Australian team showed in healthy postmenopausal women that a small dose of the male hormone testosterone prevented protein wasting. The pure crystalline testosterone, taken orally, went straight to the liver, and the dose (40mg/day) was small enough to ensure it was contained there, with no spillover to the bloodstream and other organs.
This new approach allows people to benefit from testosterone’s ability to stimulate muscle growth and increase muscle strength. At the same time, it sidesteps the side effects of testosterone when given in the usual way – administered in much larger doses by injection, gel or patch through the skin.
When testosterone is injected, it goes directly to peripheral tissues and major organs, including the brain. This can cause unwanted side effects, including aggressive behaviour and heightened libido. It can also cause heart damage, and in women induce facial hair and a deeper voice. When taken orally in a small dose, it is absorbed through the gut and goes straight to and acts on the liver, where it is also broken down, so that no other tissue or organ is exposed.
Left: Actress Suzanne Somers is the ”face” of anti-aging and rhGH.“The novel aspect of this research is that only the liver gets tickled with testosterone. It is a new way of using an old hormone” said Professor Ken Ho. “This is a great advantage because it avoids the unpleasant behavioral effects of high doses of testosterone injected into the bloodstream and the masculinizing effects in women.”“We saw that low dose testosterone, taken orally, had the same magnitude of effect on whole body protein metabolism as when it is injected in larger doses in men,” added Dr Vita Birzniece. “This is really hopeful, because if we can see the same effect on protein metabolism at this stage, we believe it will translate into the same increase in muscle mass that we see from testosterone delivered systemically, yet avoiding all the unpleasant side effects.”
Testosterone stimulates extra-hepatic but not hepatic fat oxidation (Fox): comparison of oral and transdermal testosterone administration in hypopituitary men. Birzniece V , Meinhardt UJ , Handelsman DJ , Ho KK 2009
Birzniece V , Meinhardt UJ , Handelsman DJ , Ho KK 2009
Fat mass is increased in hypogonadal men and the changes are reversed by testosterone replacement. Testosterone administration enhances whole body fat oxidation (Fox). Fat is oxidized in the liver and in extra-hepatic tissues.
The objective was to determine whether the stimulation of Fox by testosterone arises primarily from the liver or from extra-hepatic tissues.
T hirteen men with hypopituitarism, around 53 year of age, with both growth hormone (GH) and testosterone deficiency were studied sequentially after 2 weeks of treatment with transdermal testosterone (5 mg), no treatment, and stepwise incremental doses of oral crystalline testosterone (10, 20, 40 and 80 mg) in the absence of GH replacement.
hirteen men with hypopituitarism, around 53 year of age, with both growth hormone (GH) and testosterone deficiency were studied sequentially after 2 weeks of treatment with transdermal testosterone (5 mg), no treatment, and stepwise incremental doses of oral crystalline testosterone (10, 20, 40 and 80 mg) in the absence of GH replacement.
When compared to the no-treatment phase, mean blood testosterone levels rose into the physiological range after transdermal testosterone delivery but did not significantly change after 10, 20, 40 or 80 mg oral testosterone treatment. Blood SHBG and TBG fell significantly with 80 mg oral testosterone dose but were unaffected by any other testosterone treatment. Fox increased significantly with transdermal but not with any dose of oral testosterone. Mean plasma IGF-I and REE were unaffected by testosterone, regardless of the route or dose.
CONCLUSIONS: Short-term testosterone administration does not stimulate hepatic fat oxidation but enhances whole body fat oxidation by acting on extra-hepatic tissues. And doses until 40 mg/day of oral testosterone will not suppress the HPTA.
Interaction between Testosterone and Growth Hormone on Whole-Body Protein Anabolism Occurs in the Liver Birzniece, Meinhardt, Umpleby, Handelsman and Ho 2011
In adults with GH deficiency, muscle mass is reduced with these differences reversed upon GH replacement. Androgen deficiency also results in a reduction in muscle mass, which is normalized by testosterone re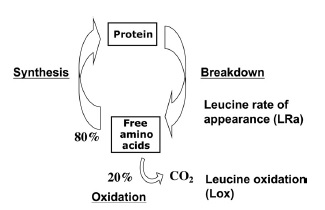 placement. Thus, GH and testosterone both exert muscle anabolic effect and may act synergistically. Evidence shows that both hormones are necessary to exert an optimal effect. This is exemplified in GH-deficient men in whom lean body mass remains subnormal even after adequate androgen replacement. Linear growth in G H-deficient children receiving GH replacement is further stimulated by androgen treatment, and for full androgen growth-promoting effect, GH replacement is required. This observation suggests that the anabolic effect of androgens may depend on the presence of GH. In pre-pubertal boys with GH deficiency, testosterone and GH replacement results in a greater stimulation of whole-body protein synthesis than testosterone treatment alone. How GH and testosterone interact to regulate protein metabolism in adult life is poorly understood. We recently reported that in hypopituitary men, both GH and testosterone promote protein anabolism, this effect being enhanced with combined treatment. Thus, testosterone and GH exert independent and additive effects in regulating protein metabolism. However, the primary site of GH and testosterone interaction is unknown.
placement. Thus, GH and testosterone both exert muscle anabolic effect and may act synergistically. Evidence shows that both hormones are necessary to exert an optimal effect. This is exemplified in GH-deficient men in whom lean body mass remains subnormal even after adequate androgen replacement. Linear growth in G H-deficient children receiving GH replacement is further stimulated by androgen treatment, and for full androgen growth-promoting effect, GH replacement is required. This observation suggests that the anabolic effect of androgens may depend on the presence of GH. In pre-pubertal boys with GH deficiency, testosterone and GH replacement results in a greater stimulation of whole-body protein synthesis than testosterone treatment alone. How GH and testosterone interact to regulate protein metabolism in adult life is poorly understood. We recently reported that in hypopituitary men, both GH and testosterone promote protein anabolism, this effect being enhanced with combined treatment. Thus, testosterone and GH exert independent and additive effects in regulating protein metabolism. However, the primary site of GH and testosterone interaction is unknown.
Liver and muscle are major sites where protein metabolism is regulated. We aimed to determine whether the site of GH and testosterone interaction on protein metabolism is primarily hepatic or extrahepatic. Oral delivery of testosterone exposes the liver to high portal levels of testosterone, which undergoes first-pass hepatic metabolism reducing or preventing the appearance of additional testosterone in the systemic circulation. We compared the impact on whole-body protein metabolism of testosterone administered via oral route (at doses used resulting in solely hepatic testosterone exposure) with transdermal testosterone replacement (systemic testosterone exposure) in the presence or absence of GH.
In this open-label randomized crossover study, the impact on whole-body protein metabolism of oral (solely hepatic testosterone exposure) and transdermal (systemic testosterone exposure) testosterone replacement in the presence or absence of GH was compared.
Eleven hypopituitary men with GH and testosterone deficiency were randomized to 2-wk treatments with transdermal testosterone (10 mg) or oral testosterone (40 mg), with or without GH replacement (0.6 mg/d [1.6 IU]).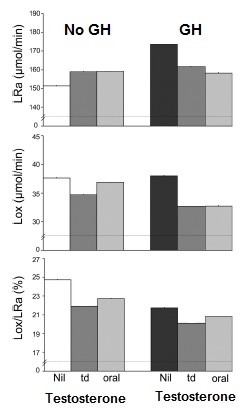 The dose of testosterone administered orally achieves physiological portal testosterone concentrations without spillover into the systemic circulation.
The dose of testosterone administered orally achieves physiological portal testosterone concentrations without spillover into the systemic circulation.
Whole-body leucine turnover was measured, from which leucine rate of appearance (LRa), an index of protein breakdown, and leucine oxidation (Lox), a measure of irreversible protein loss, were estimated at the end of each treatment.
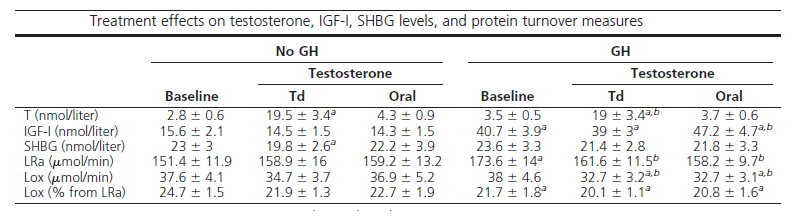
In the absence of GH, neither transdermal nor oral testosterone affected LRa or Lox. GH therapy significantly increased LRa, an effect equally reduced by transdermal and oral testosterone administration. GH replacement alone did not significantly change Lox, whereas addition of testosterone treatment reduced Lox, with the effect not significantly different between transdermal and oral testosterone.
In the doses used, testosterone stimulates protein anabolism by reducing protein breakdown and oxidation only in the presence of GH. Because the net effect on protein metabolism during GH therapy is not different between systemic and solely hepatic testosterone administration, we conclude that the liver is the primary site of this hormonal interaction.
IGF-I levels
In the absence of GH, neither transdermal nor oral testosterone administration significantly changed IGF-I levels. During GH therapy, the mean IGF-I levels significantly increased compared with baseline. GH co-administration with transdermal and oral testosterone significantly increased circulating IGF-I compared with baseline. During GH therapy, IGF-I levels significantly increased with oral but not transdermal testosterone treatment compared with GH therapy alone. The changes in circulating IGF-I levels between oral and transdermal testosterone during GH therapy but were not significantly different.
SHBG levels
In the absence of GH, mean SHBG levels on transdermal testosterone administration were significantly lower compared with baseline, whereas on oral testosterone administration, mean SHBG levels did not significantly differ from baseline.
When compared with baseline, mean SHBG levels did not significantly change during GH therapy alone or in combination with either transdermal or oral testosterone.
To summarize all this and see what it means for us.
The finding that a certain amount of oral testosterone, and thus probably other oral steroids) is not broken down during the first pass of the liver:
“The participants were studied at baseline and after 2 weeks of testosterone administration at a dose of 40 mg/day orally. Testosterone was administrated as capsules filled with crystalline testosterone U SP without excipients. The daily 40 mg dose of crystalline testosterone was divided into three doses taken every 8 h to achieve steady hepatic exposure. The dose was based on our previous work on hypogonadal men in whom 40 mg/day of oral crystalline testosterone was the highest dose that did not increase systemic levels of testosterone and did not reduce the blood levels of SHBG, indicative of an absence of pharmacological androgen effects on the liver. No significant increase in the concentration of testosterone occurred in peripheral blood, indicative of the absence of a systemic spillover.”
SP without excipients. The daily 40 mg dose of crystalline testosterone was divided into three doses taken every 8 h to achieve steady hepatic exposure. The dose was based on our previous work on hypogonadal men in whom 40 mg/day of oral crystalline testosterone was the highest dose that did not increase systemic levels of testosterone and did not reduce the blood levels of SHBG, indicative of an absence of pharmacological androgen effects on the liver. No significant increase in the concentration of testosterone occurred in peripheral blood, indicative of the absence of a systemic spillover.”
From the other studies the results that rhGH works synergistically with Testosterone, is an open door for every bodybuilder. Also that they reduce body fat.
Doses
Three daily doses with a total of 40 mg per day seems low. But the average daily production of testosterone by the Leydig cells is 3 -7mg, and a typical adult male has just 0.035 milligrams of testosterone floating around in his bloodstream. Since 40 mg doesn’t cause a spill-over in the systemic system, and therefore causes no suppression, the sum of these combined with rhGH, (much) higher than the dose of 1.6 IU used in the studies, and combined with a healthy protein-rich diet and heavy work-outs could be surprising.
Because these links often don’t work directly or via GOOGLE etc you can view these articles via TOR. So much for censorship..
https://www.juicedmuscle.com/jmblog/content/homebrewing-beta-cyclodextrins
https://juicedmuscle.com/jmblog/content/more-labscale-experiments
