
Aromasin (Exemestane) for bodycomposition improvement

Beginning this year I wrote about Aromasin**. But bodybuilders are very resourceful in  combining synergistically acting compounds. Just remember the combination AS/GH/Slin that created the first mass monsters. Thus many combine Exemestane with SERM’s, roids and GH, and get good results. Anecdotic evidence shared on the discussion forums such as bloodwork-results and individual results.
combining synergistically acting compounds. Just remember the combination AS/GH/Slin that created the first mass monsters. Thus many combine Exemestane with SERM’s, roids and GH, and get good results. Anecdotic evidence shared on the discussion forums such as bloodwork-results and individual results.
Medical scientist don’t like these kinds of self-medication and bodybuilders are known to do this, this is perhaps the reason that de Ronde in his 2011 study wrote:
“Aromatase inhibitors may be an attractive alternative for traditional testosterone substitution in elderly men because these compounds can be administered orally once daily and may result in physiological 24 h testosterone profiles. Additionally, misuse of aromatase inhibitors is unlikely since testosterone levels will not be stimulated to vastly supraphysiological levels. A small, controlled study demonstrated that anastrozole in a dose of 1 mg daily during 12 weeks will result in doubling of the mean bioavailable testosterone level in older men. A more recent study also showed a moderate but significant effect of aromatase inhibition on estradiol and testosterone levels in older men. Treatment with atamestane 100 mg once daily resulted in a 40% increase in total testosterone levels after 36 weeks. However, no beneficial effects were seen on muscle strength, body composition or quality-of-life scores. A similar increase of testosterone levels in the absence of effects on body composition and strength was reported in a study, in which elderly men with borderline low levels of serum testosterone were treated with anastrozole during 1 year.”
Handelman in a few studies thinks differently. Handelsman 2006: “Blockade of oestrogen action is, however, one form of indirect androgen doping that can stimulate sustained,  albeit modest, increases in endogenous LH secretion in physiological pulsatile patterns sufficient to maintain a modest increase in blood testosterone concentrations.”
albeit modest, increases in endogenous LH secretion in physiological pulsatile patterns sufficient to maintain a modest increase in blood testosterone concentrations.”
Handelsman 2008: “Hence it is likely that more effective oestrogen blockade in men would produce significant and sustained elevations of blood testosterone concentrations possibly sufficient to produce myotrophic and performance-enhancing effects in men treated with such drugs. Hence, despite the lack of direct ergogenic studies of oestrogen blockers in men, the available evidence provides a firm basis for the class-specific banning of oestrogen blockers in men.”
Older men
 There is a growing interest in the treatment of late-onset hypogonadism, another name for the study of testosterone deficiency in an older age group. Initial attempts at testosterone replacement have also brought attention to the possible adverse effects on the patients' cardiovascular risk factors and their prostate health. The “female” hormone estradiol is no longer considered as the feminizing hormone, as it has been identified to have an effect on the sexual and general well-being of adult males. Urologists and endocrinologists alike have started to pay attention to the serum T/E2 (testosterone : estradiol) ratio that appears to be more important than the respective individual hormonal levels. Therein lies the possible role of aromatase inhibitors (AIs) in restoring the normal balance of serum testosterone and estradiol levels for the adequate treatment of late-onset hypogonadism, while limiting the potential adverse effects.
There is a growing interest in the treatment of late-onset hypogonadism, another name for the study of testosterone deficiency in an older age group. Initial attempts at testosterone replacement have also brought attention to the possible adverse effects on the patients' cardiovascular risk factors and their prostate health. The “female” hormone estradiol is no longer considered as the feminizing hormone, as it has been identified to have an effect on the sexual and general well-being of adult males. Urologists and endocrinologists alike have started to pay attention to the serum T/E2 (testosterone : estradiol) ratio that appears to be more important than the respective individual hormonal levels. Therein lies the possible role of aromatase inhibitors (AIs) in restoring the normal balance of serum testosterone and estradiol levels for the adequate treatment of late-onset hypogonadism, while limiting the potential adverse effects.
Tan et al 2014: “Currently there is no literature to recommend the use of AIs in adult males to treat late-onset hypogonadism, obesity-related hypogonadotropic hypogonadism, gynecomastia, or male subfertility, although some positive effects have been reported. The adverse effects on bone health seen in females treated with AIs are not seen in males.
Conclusions:
With the better understanding of the T/E2 ratio in adult males, the lack of scientific data to show that bone health is adversely affected by AI usage in adult males, the positive effects of AIs on the treatment of conditions like late-onset hypogonadism and male subfertility encourages conducting large-scale, multicenter, randomized controlled trials for the clinical use of AIs in adult males.”
Clomid – Nolvadex etc
The lack of other well-proven indications and wide clinical usage of oestrogen blockers in men mean that there are few clinical efficacy or safety studies of these drugs in men. It is, nevertheless, well established that oestrogen blockers consistently increase blood testosterone concentrations in men by up to 50%. For example, in normal men, antioestrogens such as clomiphene, tamoxifen and raloxifene cause reflex increases in pituitary gonadotrophin secretion and circulating testosterone levels. Similar increases in blood testosterone concentrations ranging from 5 to 20 nmol L are reported with aromatase inhibitors such as testolactone, exemestane and anastrozole. The mechanism is most likely to be via inhibition of androgenic negative feedback on the hypothalamus, similar to the effects of antiandrogens such as flutamide or nilutamide which all cause reflex increases in blood LH and testosterone. For oestrogen blockers, the common mechanism of action—inhibiting a significant part of testosterone's hypothalamic negative feedback, which is due to aromatization—makes it highly likely that all oestrogen blockers would have similar class-wide effects, proportional to their oestrogen-blocking effectiveness.
These studies show not only dose-dependent effects of tamoxifen (in preventing gynecomastia) but also, at the highest dose (20 mg day), superiority over anastrozole (1 mg day).
Effects on muscle and fat mass
In 2008 Montagnani et al monitored 68 older women for 2 years. All the women had already been taking 20 mg tamoxifen daily for 2-3 years. Half of them continued with this and the other half started taking 25 mg exemestane per day instead.
ResultsThe exemestane group built up lean body mass. In the two years that the trial lasted the women in that group gained an average of 2.2 kg lean body mass. And the same group lost an average of 0.7 kg fat. The figures below show the effects as a percentage.
The triglyceride levels in the blood of the women in the exemestane group went down – a positive development. At the same time exemestane increased the levels of LDL [bad cholesterol] and reduced the concentration of HDL [good cholesterol] – a negative development. Bodybuilders of course add tamoxifen and supplements to counteract the bad change in bloodlipids.
Experimentally Determined Binding of 17-Hydroexemestane and Exemestane to ERα and AR
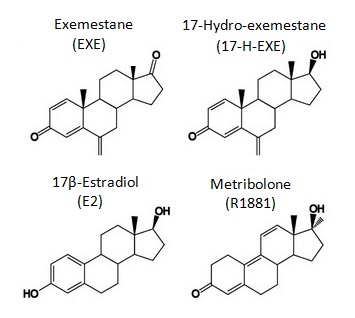 Structures of the compounds relevant to these studies, the steroidal AI parent compound exemestane, its primary metabolite 17-hydroexemestane, E2, and the synthetic non-aromatizable androgen R1881.
Structures of the compounds relevant to these studies, the steroidal AI parent compound exemestane, its primary metabolite 17-hydroexemestane, E2, and the synthetic non-aromatizable androgen R1881.
Importantly, the only difference between parental exemestane (EXE) and its metabolite 17-hydroexemestane is a hydroxyl group in the metabolite in place of a ketone in the parent compound at the 17β position, whereas both compounds share a 3-keto group.
For steroidal estrogens, elimination or modification of the 17β-OH group reduces binding to ERα, but that of the 3-OH group is much more dramatic. For steroidal androgens, the trend is reversed; elimination or modification of the 17β-OH group is more significant for AR binding than that of the 3-keto group. The 3-keto group found in both exemestane and 17-hydroexemestane also favors binding to AR.
Receptor binding assay’s
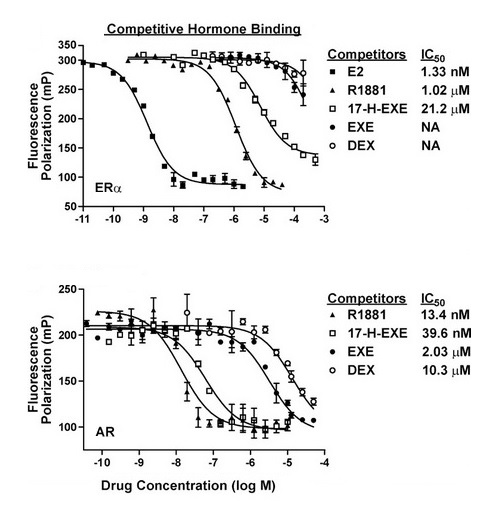 Unlike nonsteroidal AIs, the steroidal AI exemestane may exert beneficial effects on bone through its primary metabolite 17-hydroexemestane. We investigated 17-hydroexemestane and observed it bound estrogen receptor alpha (ERalpha) very weakly and androgen receptor (AR) strongly.
Unlike nonsteroidal AIs, the steroidal AI exemestane may exert beneficial effects on bone through its primary metabolite 17-hydroexemestane. We investigated 17-hydroexemestane and observed it bound estrogen receptor alpha (ERalpha) very weakly and androgen receptor (AR) strongly.
Responses of each cell type to high and low concentrations of the non-aromatizable synthetic androgen R1881 (Metribolone) paralleled those of 17-hydroexemestane. 17-Hydroexemestane down-regulated ERalpha protein levels at high concentrations in a cell type-specific manner similarly as 17beta-estradiol, and increased AR protein accumulation at low concentrations in both cell types similarly as R1881.
Computer docking indicated that the 17beta-OH group of 17-hydroexemestane relative to the 17-keto group of exemestane contributed significantly more intermolecular interaction energy toward binding AR than ERalpha. Molecular modeling also indicated that 17-hydroexemestane interacted with ERalpha and AR through selective recognition motifs employed by 17beta-estradiol and R1881, respectively. We conclude that 17-hydroexemestane exerts biological effects as an androgen. These results may have important implications for long-term maintenance of patients with AIs.
"Pharmacokinetics and Dose Finding of a Potent Aromatase Inhibitor, Aromasin (Exemestane), in Young Males"
Suppression of estrogen, via estrogen receptor or aromatase blockade, is being investigated in the treatment of different conditions. Exemestane (Aromasin) is a potent and selective irreversible aromatase inhibitor. To characterize its suppression of estrogen and its pharmacokinetic properties in young healthy males. In a cross-over study, 12 were randomly assigned to 25 and 50 mg exemestane daily, orally, for 10 days with a 14-day washout period. Blood was withdrawn before and 24 hour after the last dose of each treatment period.
These are the results of the first detailed study of the pharmacological effects of exemestane in male (!!!!) subjects. Doses of 25 and 50 mg were comparable in  suppressing all circulating estrogens and had similar effects of increasing serum androstenedione and testosterone concentrations. There were mean 38%, 71%, and 45% decreases in estradiol, estrone, and estrone sulfate concentrations, respectively, after 10 days, approximately 24 hours after administration of the last dose of 25 mg exemestane, coupled with 60% increases in testosterone and 32% increases in androstenedione concentrations. The rise in the aromatase substrates, testosterone and androstenedione, is probably secondary to substrate accumulation and/or to the feedback increase in gonadotropins caused by aromatase blockade.
suppressing all circulating estrogens and had similar effects of increasing serum androstenedione and testosterone concentrations. There were mean 38%, 71%, and 45% decreases in estradiol, estrone, and estrone sulfate concentrations, respectively, after 10 days, approximately 24 hours after administration of the last dose of 25 mg exemestane, coupled with 60% increases in testosterone and 32% increases in androstenedione concentrations. The rise in the aromatase substrates, testosterone and androstenedione, is probably secondary to substrate accumulation and/or to the feedback increase in gonadotropins caused by aromatase blockade.
SHBG concentrations were decreased by a mean 21% and 19% at 25 and 50 mg exemestane, respectively.
At the end of the 10 days, total testosterone had increased ~60%, but free testosterone (that is, the testosterone that is actually free to bind the androgen receptor ) increased by 117%!!!
The reason this works is because estrogen is reduced as a result of the aromatase blockage, and estrogen is the main negative feedback signal to the hypothalamus to decrease LH secretion. So with lower estrogen in the system, more LH is secreted and more testosterone is made. It’s a double whammy as well, because with aromatase blockage, less testosterone is lost in the conversion to estrogen.
Whether or not this increased testosterone will result in anabolic affects however is up for debate. Seen the posted studies above on the binding and potency of 17-hydroexemestane makes a difference.
Note in the first study, estrogen levels returned to normal 3-6 days after aromasin withdrawal, so the drug must be continuously taken to keep the increased levels of testosterone.
The terminal half-life in the present study (~9 hours) was considerably shorter than the published value of 27 hours (in postmenopausal women). The reason for this difference is not clear, but may be related to a true gender dependency possibly involving the volume of distribution (lower in males than females) and plasma or tissue protein binding (respectively, higher and lower in males). 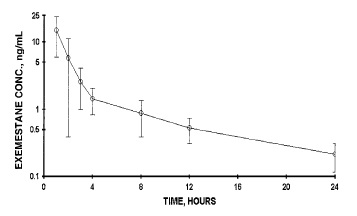
The maximal suppression evoked by exemestane at the single dose of 25 mg in the present study was similar to published results in postmenopausal women, but the time course differed. Evans et al. (reported that a single 25-mg oral dose of exemestane maximally suppressed estradiol concentrations by 72% 3 d after administration, and estradiol levels returned to baseline only 8–11 d after drug administration.
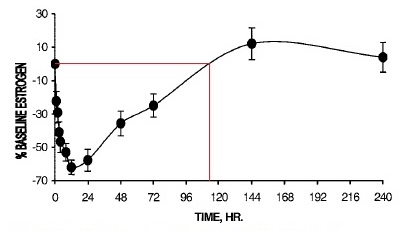 Graph: Percent change from baseline in plasma estradiol concentrations after a single 25-mg dose of exemestane in 10 young men.
Graph: Percent change from baseline in plasma estradiol concentrations after a single 25-mg dose of exemestane in 10 young men.
In the present study maximal suppression of estradiol of 62% was observed 12 hours after exemestane administration and returned to baseline 3–6 d after administration.
The reason for this difference is not clear, but may be related to the shorter half-life of exemestane in males, the lower exposure to exemestane, and the higher levels of the aromatase substrates androstenedione (1 ng/ml in young males vs. 0.5 ng/ml in postmenopausal women), particularly the much higher testosterone concentrations in young males than in postmenopausal women (700 ng/dl vs. 20 ng/dl, respectively) (25). This is supported by the observation that in the 10-d study in young males reported here, the suppression of estradiol is weaker (due to the very high levels of the precursor testosterone) than that of estrone (due to androstenedione levels not very different from those in postmenopausal women).
Effects of aromatase inhibition in obese men
Peripheral androgen aromatization is enhanced in subjects with increased body mass index. Massively obese men show markedly increased plasma estradiol concentrations and low testosterone concentrations . In three small studies, letrozole or testolactone has been administered to morbidly obese men to improve their testosterone levels. Treatment resulted in normalization of testosterone levels in all subjects, with a concomitant suppression of the originally increased levels of estradiol. This normalization of the estradiol/testosterone ratio might be of advantage, because of the suppressive effects of testosterone on the expression of the  estrogen receptor β, which in itself, in the presence of high levels of estradiol, can suppress the expression of GLUT-4, leading to insulin insensitivity. A case study describes a morbidly obese infertile man, who after a similar treatment with anastrozole showed a normalized pituitary-testis axis, spermatogenesis and fertility. However, testosterone levels will also improve on weight loss, which is the intervention of choice for obese men with or without low testosterone levels. In fact another recent report even suggested aromatase inhibitors may be of benefit to obese men who suffer from hypogonadism due to the excess estrogen that usually accompanies obesity.
estrogen receptor β, which in itself, in the presence of high levels of estradiol, can suppress the expression of GLUT-4, leading to insulin insensitivity. A case study describes a morbidly obese infertile man, who after a similar treatment with anastrozole showed a normalized pituitary-testis axis, spermatogenesis and fertility. However, testosterone levels will also improve on weight loss, which is the intervention of choice for obese men with or without low testosterone levels. In fact another recent report even suggested aromatase inhibitors may be of benefit to obese men who suffer from hypogonadism due to the excess estrogen that usually accompanies obesity.
Exemestane vs Tamoxifen on blood lipids
 Exemestane appears to have a neutral effect on total cholesterol and HDL levels. Unlike tamoxifen's positive effect on LDL levels, exemestane does not significantly alter LDL levels. Tamoxifen on the other hand increases triglyceride levels, while exemestane results in a beneficial reduction in TRG levels. These data offer additional information with regard to the safety and tolerability of exemestane in postmenopausal breast cancer patients and support further investigation of its potential usefulness in the adjuvant setting.
Exemestane appears to have a neutral effect on total cholesterol and HDL levels. Unlike tamoxifen's positive effect on LDL levels, exemestane does not significantly alter LDL levels. Tamoxifen on the other hand increases triglyceride levels, while exemestane results in a beneficial reduction in TRG levels. These data offer additional information with regard to the safety and tolerability of exemestane in postmenopausal breast cancer patients and support further investigation of its potential usefulness in the adjuvant setting.
Dosing
A funny phrase from a discussion forum: “The best gage I have found to control your Estradiol levels is to gage your night time and morning wood. At good levels or what I call the sweet spot you get your night time and morning wood back so strong it will wake you up and you can hang a coat on it.”
 Dosing is individual, that is true for roids and also for anti-e or aromatase inhibitors. It also depends on other variables like gender, cycle, cycle length, height/weight etc. On light cycles 12.5mg Aromasin twice a week should be enough to regulate estrogen levels while increasing overall testosterone.
Dosing is individual, that is true for roids and also for anti-e or aromatase inhibitors. It also depends on other variables like gender, cycle, cycle length, height/weight etc. On light cycles 12.5mg Aromasin twice a week should be enough to regulate estrogen levels while increasing overall testosterone.
Aromasin is actually quite a safe drug, with minimal side effects.
Exemestane's half-life in the male body is actually very short (~9 hours) and it is quickly eliminated, however, since as soon as it enters your bloodstream it quickly destroys 80-90% of the aromatase enzymes present in your body, it is effective in maintaining significant reductions in estrogen for up to 72 hours after a single 25mg dose. Estrogen levels only begin to rise again after your body has begun to make new aromatase enzymes to replace the ones destroyed by exemestane.
-24 hours after one 25mg dose estrogen levels are reduced by 70-80%-72 hours later estrogen levels are still 40% below baseline even though the drug itself is almost completely eliminated
-120 hours after initial dose estrogen levels return to baseline (without rebounding)-this  means that you can find the timing and dosage that works for you, I’ve seen some guys recommend between 25mg ED(every day) and 12.5mg e4d, and you can see why both are effective while providing different levels of estrogen suppression, and it is this flexibility that makes exemestane such a versatile anti-e.
means that you can find the timing and dosage that works for you, I’ve seen some guys recommend between 25mg ED(every day) and 12.5mg e4d, and you can see why both are effective while providing different levels of estrogen suppression, and it is this flexibility that makes exemestane such a versatile anti-e.
If you use not enough you will bloat and/or lose your libido. If you use to much you will suffer stiff joints. Many guys will tell you if you are using the right amount you will experience a feeling of wellbeing. And like I posted above - your morning erections.